

Chronic Kidney Disease or Hypertension After Childhood Cancer
- PMID: 40388170
- PMCID: PMC12090035
- DOI: 10.1001/jamanetworkopen.2025.8199
Chronic Kidney Disease or Hypertension After Childhood Cancer
Abstract
Importance: Post-cancer therapy kidney outcomes, including chronic kidney disease (CKD) and hypertension, are common in childhood cancer survivors (CCS). The incidence and timing of CKD and hypertension in CCS compared with other at-risk or general populations are unclear.
Objective: To determine the association of childhood cancer treatment with post-cancer therapy CKD or hypertension.
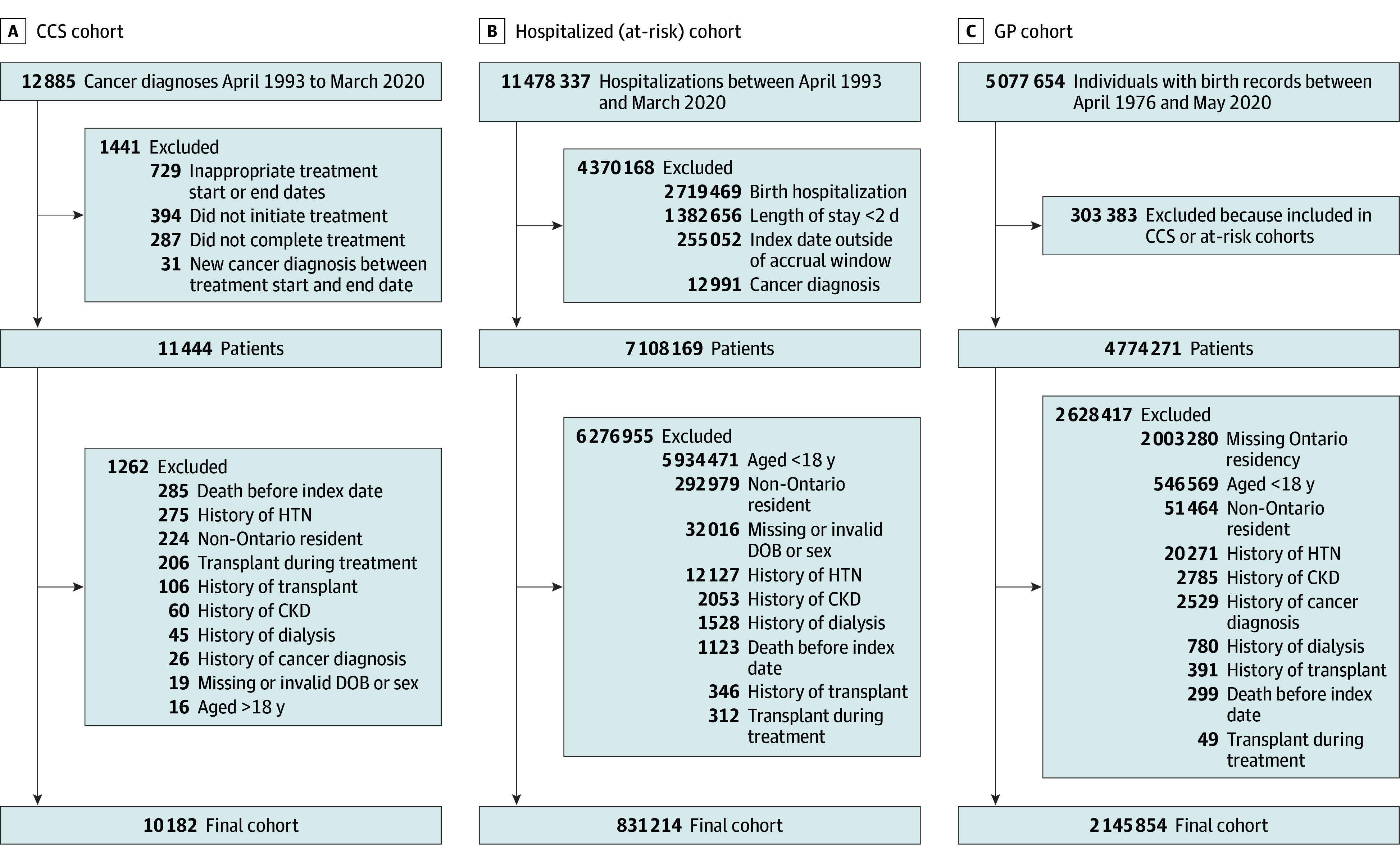
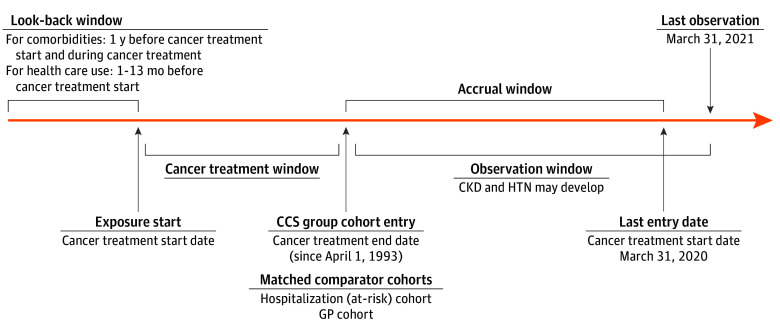
Design, setting, and participants: Population-based matched cohort study of children treated for cancer between April 1993 and March 2020 in Ontario, Canada, with follow-up until March 2021. The CCS (exposed) cohort included children (≤18 years) surviving cancer. Comparator cohorts were a hospitalization cohort (children who were hospitalized) and a general pediatric population (GP) cohort (all other Ontario children). Exclusion criteria were history of previous cancer, organ transplant, CKD, dialysis, or hypertension. Matching with each of the 2 comparator cohorts was performed separately and in a 1:4 ratio by age, sex, rural vs urban status, income quintile, index year, and presence of previous hospitalization. Data were analyzed from March 2021 to August 2024.
Exposure: Treatment for cancer.
Main outcomes and measures: The primary outcome was the composite of CKD or hypertension, defined by administrative health care diagnosis and procedure codes. Fine and Gray subdistribution hazard modeling, accounting for competing risks (death and new cancer diagnosis or relapse) and adjusting for cardiac disease, liver disease, and diabetes, was used to determine the association of cancer treatment with outcomes.
Results: There were 10 182 CCS (median [IQR] age at diagnosis, 7 [3-13] years; 5529 male [54.3%]; median [IQR] follow-up time, 8 [2-15] years) matched to 40 728 hospitalization cohort patients (median [IQR] age at diagnosis, 7 [2-12] years; 5529 male [weighted percentage, 54.3%]; median [IQR] follow-up time, 11 [6-18] years) and 8849 CCS (median [IQR] age at diagnosis, 5 [2-11] years; 4825 male [54.5%]; median [IQR] follow-up time, 7 [2-14] years) matched to 35 307 GP cohort individuals (median [IQR] age at diagnosis, 6 [2-11] years; 4825 male [weighted percentage, 54.5%]; median [IQR] follow-up time, 10 [5-16] years). Most frequent cancer types were leukemia (2948 patients [29.0%]), central nervous system neoplasms (2123 patients [20.9%]), and lymphoma (1583 patients [15.5%]). During observation, cumulative incidence of CKD or hypertension was 20.85% (95% CI, 18.75%-23.02%) in the CCS cohort vs 16.47% (95% CI, 15.21%-17.77%) in the hospitalization cohort and 19.24% (95% CI, 15.99%-22.73%) in the CCS cohort vs 8.05% (95% CI, 6.76%-9.49%) in the GP cohort. CCS were at increased risk of CKD or hypertension compared with the hospitalization cohort (adjusted hazard ratio, 2.00; 95% CI, 1.86-2.14; P < .001) and the GP cohort (adjusted hazard ratio, 4.71; 95% CI, 4.27-5.19; P < .001).
Conclusions and relevance: In this population-based study, CCS were at increased risk for CKD and hypertension, which are associated with mortality, suggesting that early detection and treatment of these conditions in CCS may decrease late complications and mortality.
Conflict of interest statement
Figures
References
-
- Botta L, Gatta G, Capocaccia R, et al. ; EUROCARE-6 Working Group . Long-term survival and cure fraction estimates for childhood cancer in Europe (EUROCARE-6): results from a population-based study. Lancet Oncol. 2022;23(12):1525-1536. - PubMed
-
- Schindler M, Belle FN, Grotzer MA, von der Weid NX, Kuehni CE; Swiss Paediatric Oncology Group (SPOG) . Childhood cancer survival in Switzerland (1976-2013): time-trends and predictors. Int J Cancer. 2017;140(1):62-74. - PubMed
-
- Erdmann F, Frederiksen LE, Bonaventure A, et al. . Childhood cancer: Survival, treatment modalities, late effects and improvements over time. Cancer Epidemiol. 2021;71(Pt B):101733. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
