

Supporting evidence-based decisions about the geographic and demographic extensions of seasonal malaria chemoprevention in Benin: A modelling study
- PMID: 40388419
- PMCID: PMC12088001
- DOI: 10.1371/journal.pgph.0004509
Supporting evidence-based decisions about the geographic and demographic extensions of seasonal malaria chemoprevention in Benin: A modelling study
Abstract
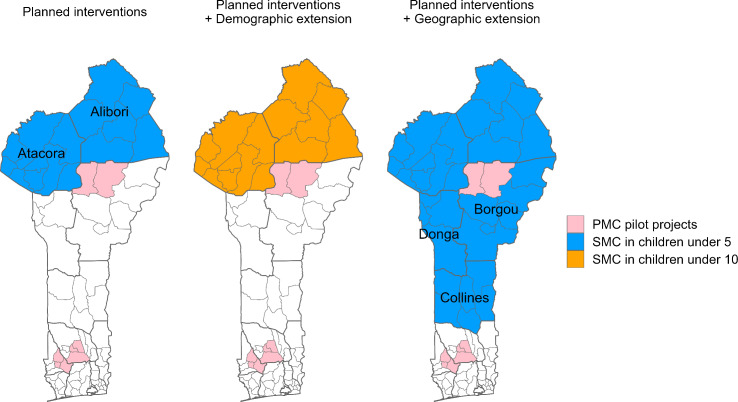
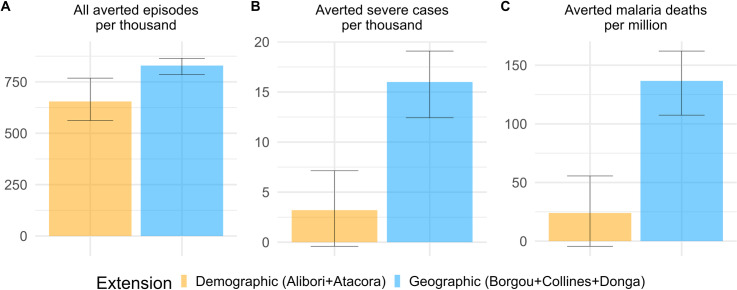
Seasonal malaria chemoprevention (SMC) has been implemented yearly in northern Benin since 2019 to reduce the malaria burden in children under 5 years of age. Its geographic scope was progressively extended until in 2022 two different extensions of SMC were considered: either demographic - children aged 5-10 in the currently targeted departments would also receive SMC, or geographic to children under 5 in new eligible departments to the south. As SMC had neither been implemented in the areas nor in the age groups suggested for expansion, modelling was used to compare the likely impact of both extensions. The model OpenMalaria was calibrated to represent the history of malaria interventions and transmission risk in administrative units of Benin. Currently planned future interventions and two scenarios for SMC extensions were simulated to inform where impact would be the highest. The model predicted that between 2024 and 2026 the geographic extension of SMC would avert at least four times more severe malaria cases and five times more direct malaria deaths per targeted child than the demographic extension. Indeed, most severe cases are concentrated in children under 5 in all departments of interest, as malaria burden remains high in this region. Numbers of severe cases averted per targeted child were similar between health zones eligible for geographic extension. The main limitations of this work are global model parameters due to lack of country-specific data on efficacy of interventions or development of immunity. SMC coverage was assumed to be uniform across rounds, zones, and age groups. Due to the high malaria burden in northern and central Benin, the geographic extension would be more impactful than the demographic extension both in absolute number of severe cases averted and per child protected, and has started to be implemented in 2024. Health zones were prioritised by availability of community health workers to deliver SMC. Mathematical modelling was a supportive tool to understand the relative impact of the different proposed SMC extensions and contributed to the decision-making process. Its integration significantly enhanced the utilisation of data for decision-making purposes. Rather than being used for forecasting, the model provided qualitative guidance that complemented other types of evidence.
Copyright: © 2025 Lemant et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
-
- World malaria report 2024: addressing inequity in the global malaria response. Geneva: World Health Organization; 2024.
-
- World Health Organization. WHO guidelines for malaria, 3 June 2022. Geneva: World Health Organization; 2022. Contract No.: WHO/UCN/GMP/2022.01 Rev.2.
-
- World Health Organization. Seasonal Malaria Chemoprevention with Sulfadoxine-Pyrimethamine Plus Amodiaquine in Children: A Field Guide. 2nd ed. Geneva: World Health Organization; 2023.
LinkOut - more resources
Full Text Sources