

Time in Target Range of Systolic Blood Pressure and Cardiovascular Disease in Patients with Chronic Kidney Disease: A Korean Nationwide Cohort Study
- PMID: 40388908
- PMCID: PMC12176353
- DOI: 10.1159/000546380
Time in Target Range of Systolic Blood Pressure and Cardiovascular Disease in Patients with Chronic Kidney Disease: A Korean Nationwide Cohort Study
Abstract
Introduction: Time in target range of systolic blood pressure (SBP-TTR) is the percentage of time that the SBP remains within 110-130 mm Hg. The association between the SBP-TTR and clinical outcomes in patients with chronic kidney disease (CKD) remains unclear. We evaluated the risks of cardiovascular disease (CVD), all-cause mortality, and renal events across the SBP-TTR groups.
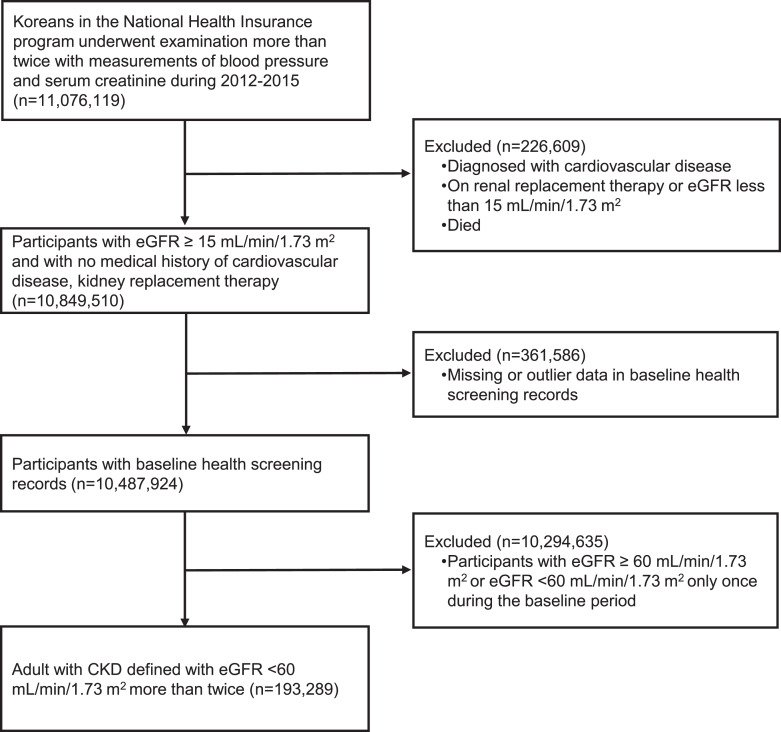
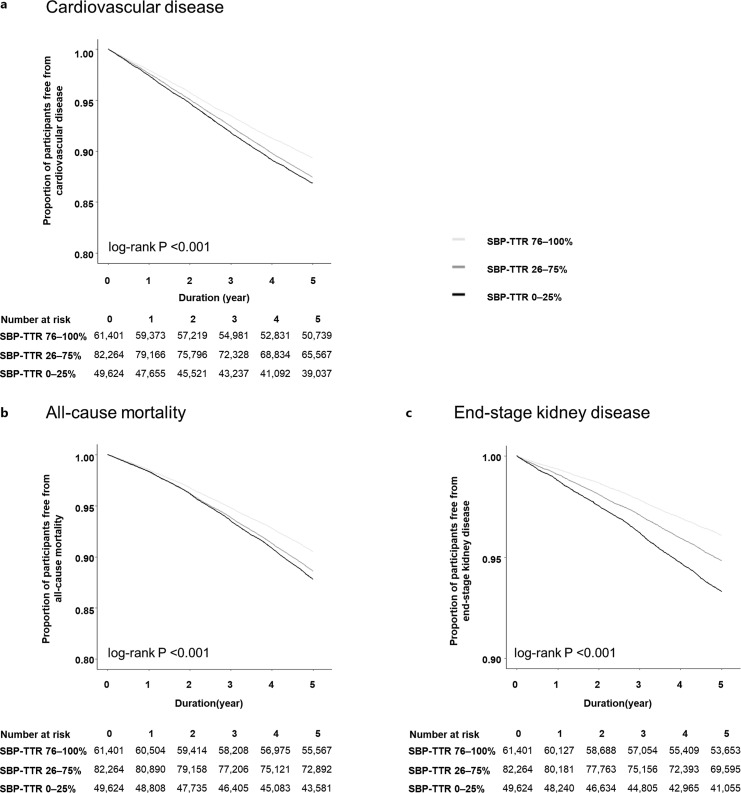
Methods: Overall, 193,289 patients with CKD who underwent at least two health checkups between 2012 and 2015 were selected from the Korean National Health Insurance Database. The patients were categorized into three categories based on their SBP-TTR levels: 76-100%, 26-75%, and 0-25%. The primary outcome was CVD risk and the secondary outcomes were all-cause mortality and progression to end-stage kidney disease (ESKD) according to SBP-TTR using Cox regression analysis.
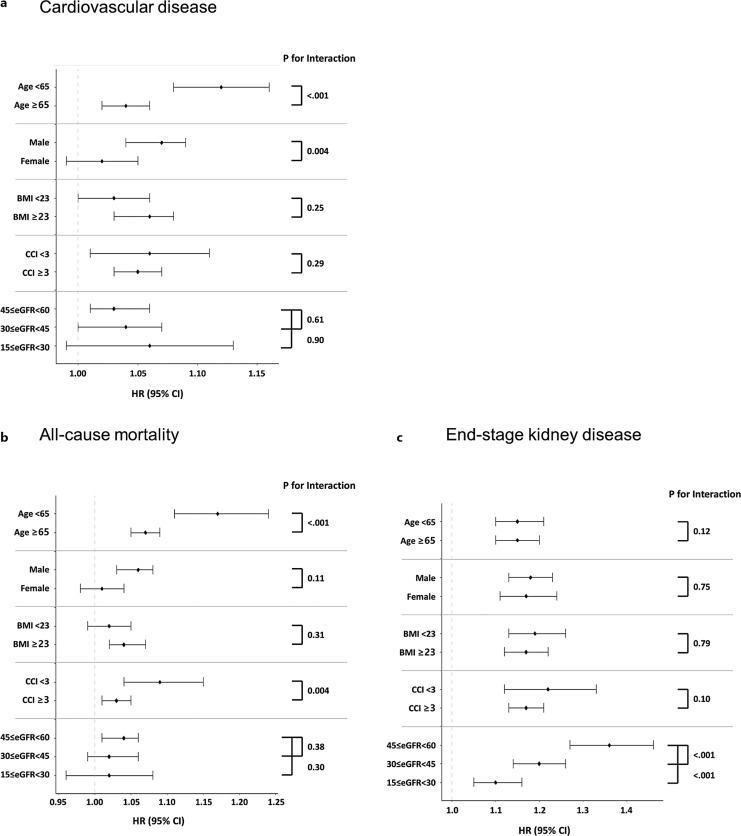
Results: Compared with patients with SBP-TTR of 76-100%, the adjusted hazard ratios (HRs) for CVD were 1.07 (95% confidence interval [CI], 1.03-1.10) and 1.09 (95% CI: 1.06-1.13) for patients with SBP-TTR of 26-75%, and 0-25%, respectively. The adjusted HR for all-cause mortality was 1.04 (95% CI: 1.003-1.07) and 1.37 (95% CI: 1.28-1.46) for patients with SBP-TTR of 26-75% and 0-25%, respectively. The adjusted HRs for ESKD progression increased gradually: 1.14-fold (95% CI: 1.07-1.21) for the SBP-TTR 26-75% group and 1.37-fold (95% CI: 1.28-1.46) for the SBP-TTR 0-25% group. For patients not taking antihypertensive medications, a lower SBP-TTR was associated with a higher risk of CVD events and ESKD progression than in those taking antihypertensive medications.
Conclusion: Among patients with CKD, those with a lower SBP-TTR had a higher risk of cardiovascular events, mortality, and progression to ESKD.
Keywords: All-cause mortality; Cardiovascular disease; Chronic kidney disease; End-stage kidney disease; Time in target range.
© 2025 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Long-Term Systolic Blood Pressure Time in Target Range and Cardiovascular Disease in Individuals With Hypertension.JACC Adv. 2025 Jun;4(6 Pt 2):101702. doi: 10.1016/j.jacadv.2025.101702. Epub 2025 Apr 16. JACC Adv. 2025. PMID: 40243985 Free PMC article.
-
Time in Target Range for Blood Pressure and Adverse Health Outcomes: A Systematic Review.Hypertension. 2025 Mar;82(3):419-431. doi: 10.1161/HYPERTENSIONAHA.124.24013. Epub 2025 Jan 13. Hypertension. 2025. PMID: 39801461
-
Patterns of systolic blood pressure response at the end of exercise and mortality and morbidity in patients referred for exercise testing.Open Heart. 2025 Mar 3;12(1):e003246. doi: 10.1136/openhrt-2025-003246. Open Heart. 2025. PMID: 40032610 Free PMC article.
-
Time in Target Range, All-Cause Mortality, and Cardiovascular Diseases.Am J Hypertens. 2025 Jul 15;38(8):537-543. doi: 10.1093/ajh/hpae144. Am J Hypertens. 2025. PMID: 39945143
-
Prenatal administration of progestogens for preventing spontaneous preterm birth in women with a multiple pregnancy.Cochrane Database Syst Rev. 2019 Nov 20;2019(11):CD012024. doi: 10.1002/14651858.CD012024.pub3. Cochrane Database Syst Rev. 2019. PMID: 31745984 Free PMC article.
References
-
- Cockwell P, Fisher L-A. The global burden of chronic kidney disease. Lancet. 2020;395(10225):662–4. - PubMed
-
- Cheung AK, Chang TI, Cushman WC, Furth SL, Hou FF, Ix JH, et al. Executive summary of the KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 2021;99(3):559–69. - PubMed
-
- Ruggenenti P, Perna A, Loriga G, Ganeva M, Ene-Iordache B, Turturro M, et al. Blood-pressure control for renoprotection in patients with non-diabetic chronic renal disease (REIN-2): multicentre, randomised controlled trial. Lancet. 2005;365(9463):939–46. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
