

Atypical ductal hyperplasia diagnosed by US-guided core needle biopsy: clinical, pathological and US features associated with upgrading to malignancy
- PMID: 40389848
- PMCID: PMC12087217
- DOI: 10.1186/s12880-025-01707-z
Atypical ductal hyperplasia diagnosed by US-guided core needle biopsy: clinical, pathological and US features associated with upgrading to malignancy
Abstract
Background: To develop a predictive model to identify atypical ductal hyperplasia (ADH) that was underestimated by US-guided core needle biopsy (CNB) and to evaluate the risk factors for underestimation for ADH with intraductal papilloma diagnosed by CNB.
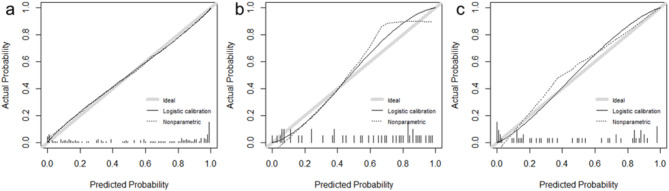
Methods: In this retrospective study, 300 CNB-diagnosed ADH lesions in 291 consecutive women between January 2014 and July 2023 were included and divided into training set (n = 181), internal validation set (n = 54), and external validation set (n = 65). The review included clinical, pathological, and US features, as well as final outcomes. Multivariate logistic regression was employed to establish predictive model and to evaluate risk factors. Model performance was evaluated using area under the receiver operating characteristic curve (AUC), calibration curve, decision curve analysis, and utility (patient stratification into low and high-risk groups). Model was validated both internally and externally by calculating its performance on validation sets.
Results: The upgrade rate to malignancy was 51.0%. Predictors included in the model were age, the pathological pattern of ADH with intraductal papilloma or ADH alone, Ki-67 positivity, and imaging-pathological discordance. The AUC was 0.915 (95% CI: 0.858, 0.955) in the training set, 0.906 (95% CI: 0.785, 0.972) in the internal validation set, and 0.934 (95% CI: 0.836, 0.983) in the external validation set. Using a cutoff value of 0.11, 38.3% of nonmalignant lesions in the training set were stratified into low-risk group with an upgrade rate of 4.1%. Similar results were obtained in the validation sets. For ADH with intraductal papilloma, age and imaging-pathological discordance were the independent risk factors for malignancy upgrading.
Conclusions: The model established to predict ADH upgrading can help in individualized risk management. If predictors of non-upgraded ADH lesions can be confirmed with larger studies, more than one-third of non-malignant lesions are expected to be candidates for non-excision.
Trial registration: This is a retrospective study.
Keywords: Atypical ductal hyperplasia; Biopsy; Breast neoplasms; Ultrasound.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This retrospective study was approved by the Medical Ethics Committee of Chinese PLA General Hospital (No. S2021-683-01). Informed consent was waived because of the retrospective design. The study was performed in accordance with the Declaration of Helsinki. Consent for publication: All authors gave their approval for manuscript’s publication. As a retrospective study, patient informed consent (e.g., reproduced images) was waived. Competing interests: The authors declare no competing interests.
Figures






References
-
- Lakhani S, Ellis I, Schnitt S, Tan P, Mj VDV. World health organization classification of tumours of the breast. Lyon: International Agency for Research on Cancer; 2012.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
