

Stress hyperglycemia ratio linked to all-cause mortality in critically ill patients with ischemic heart disease
- PMID: 40389863
- PMCID: PMC12087200
- DOI: 10.1186/s12872-025-04831-4
Stress hyperglycemia ratio linked to all-cause mortality in critically ill patients with ischemic heart disease
Abstract
Background: The stress hyperglycaemia ratio (SHR), a quantitative indicator of hyperglycaemia in stress, has been shown to correlate with poor disease prognosis. However, the relationship between SHR and short-term prognosis in critically ill patients with ischemic heart disease (IHD) remains unclear.
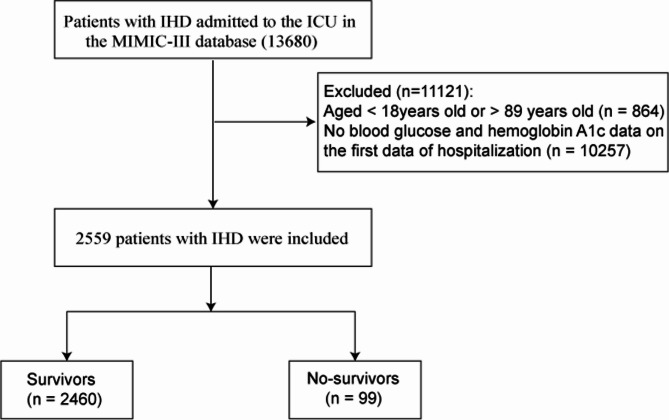
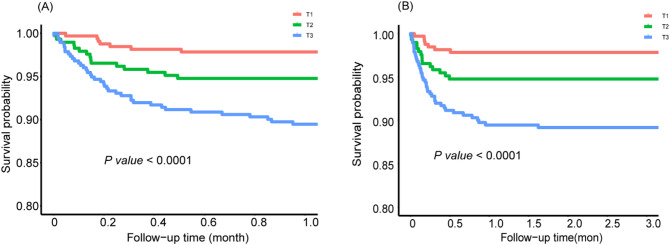
Methods: This retrospective study analyzed data of 2559 critically ill patients with IHD from the Medical Information Mart for Intensive Care III database. Endpoints were in-hospital mortality and intensive care unit (ICU) mortality. Kaplan-Meier survival curves, Cox proportional hazards models, restricted cubic spline, subgroup analysis, and receiver operating characteristic curves were used to explore the association between SHR and mortality in critically ill patients with IHD.
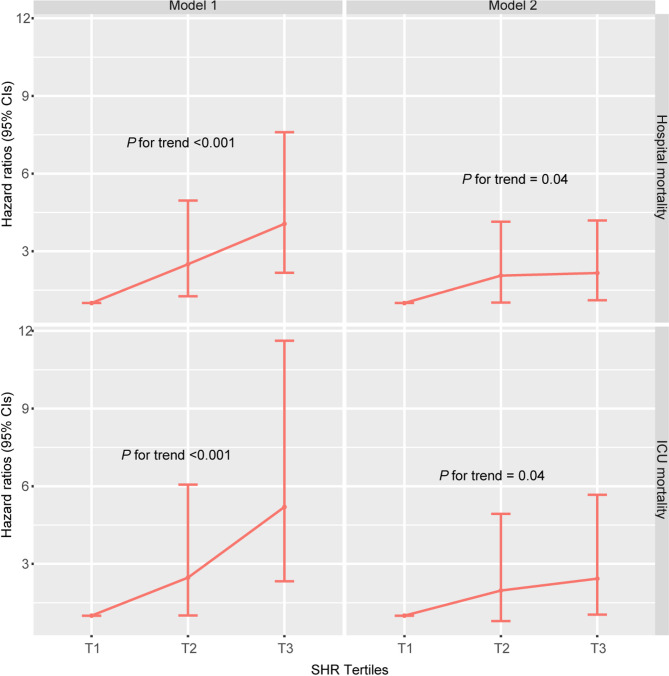
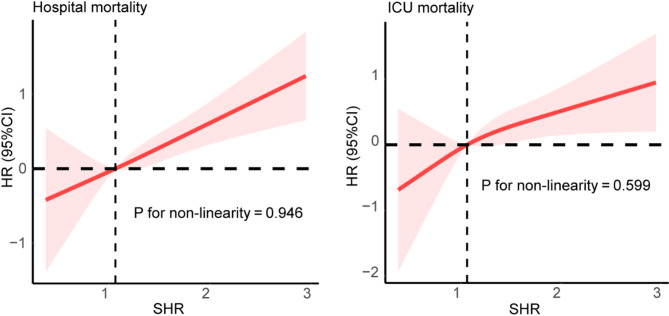
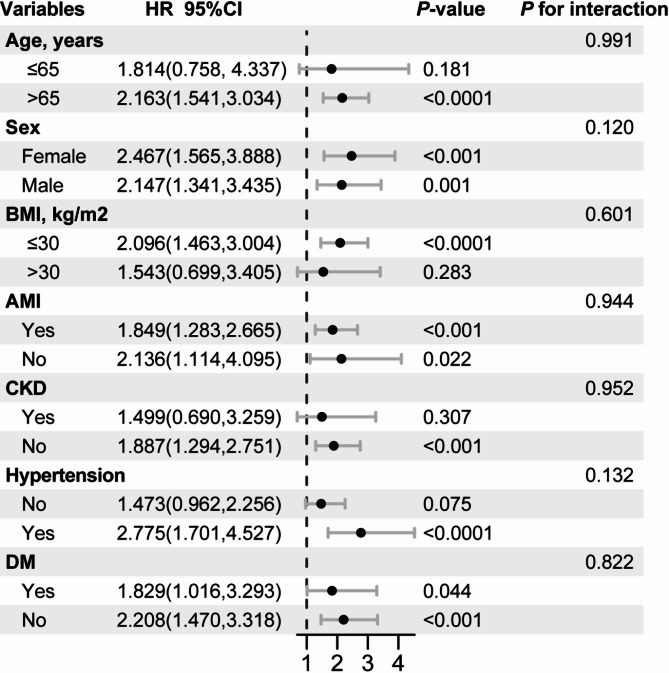
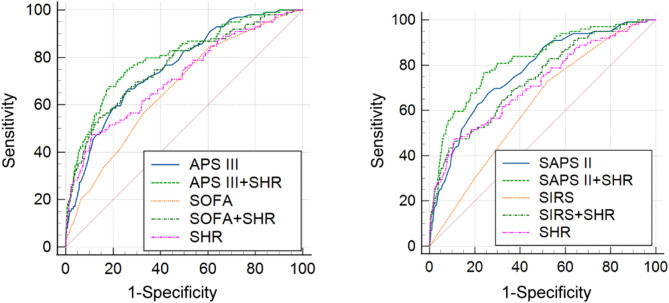
Results: A total of 99 (3.87%) in-hospital deaths and 62 (2.42%) ICU deaths were recorded. In multivariate Cox proportional hazards models, higher SHR was independently associated with in-hospital mortality (hazard ratio (HR): 1.93 [95% confidence interval (CI): 1.42-2.61], P-value < 0.0001) and ICU mortality (HR, 1.70; 95% CI, 1.17-2.47; P-value = 0.01). Restricted cubic splines showed that SHR was linearly positive correlated with both in-hospital mortality and ICU mortality. Subgroup analysis revealed the robustness of the results. The area under the curve of SHR for predicting in-hospital mortality and ICU mortality was 0.715 and 0.711, respectively.
Conclusion: SHR was significantly positively correlated with in-hospital mortality and ICU mortality in patients with critical IHD. It might enhance the predictive accuracy of existing clinical disease scores and guide personalized blood glucose control.
Keywords: Ischemic heart disease; MIMIC-III database; Mortality; Stress hyperglycemia ratio.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Consent for publication: Not applicable, this study did not contain any details, images, or videos relating to an individual person. Ethics and consent to participate declarations: The establishment of the MIMIC III database was approved by the review boards of the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center, and informed consent was obtained for all patients. Therefore, no additional ethical approval statement and informed consent requirements were required for this study. Conflict of interest: All authors have no competing interests. Clinical trial number: Not applicable.
Figures
References
-
- Shu T, Huang J, Deng J, Chen H, Zhang Y, Duan M, Wang Y, Hu X, Liu X. Development and assessment of scoring model for ICU stay and mortality prediction after emergency admissions in ischemic heart disease: a retrospective study of MIMIC-IV databases. Intern Emerg Med. 2023;18(2):487–97. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
