

Who pays more? Exploring cost disparities in medication abortion access across socio-demographic groups in Ghana
- PMID: 40390038
- PMCID: PMC12090411
- DOI: 10.1186/s12939-025-02500-8
Who pays more? Exploring cost disparities in medication abortion access across socio-demographic groups in Ghana
Abstract
Background: Medication abortion (MA) may be accessed covertly in private pharmacies and clinics due to abortion-related stigma. Stigmatization may lead to information asymmetry, resulting in price discrimination. The existing literature on abortion in Ghana has primarily focused on factors associated with abortion stigma. However, the potential variations in MA cost have not been explored. Thus, we aim to explore the potential disparities in MA cost based on women's socio-demographic status in Ghana.
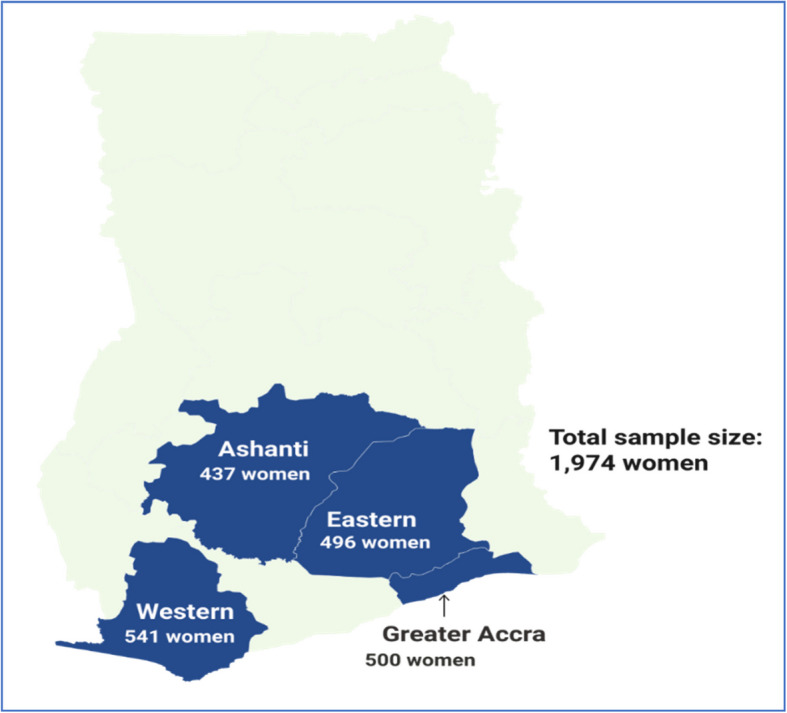
Methods: We used data from a study that recruited women who accessed MA using mifepristone and misoprostol combination from selected private pharmacies and clinics in Ghana. The study employed a non-inferiority and prospective design, and women were recruited as they exited the selected facilities after obtaining the MA pills. Our final analysis included 929 pharmacy clients and 1,045 clinic clients. To understand the variability in MA cost, we initially conducted two decomposition analyses using the variance and Blinder-Oaxaca techniques, followed by linear regressions to identify the socio-demographic factors that predict MA cost.
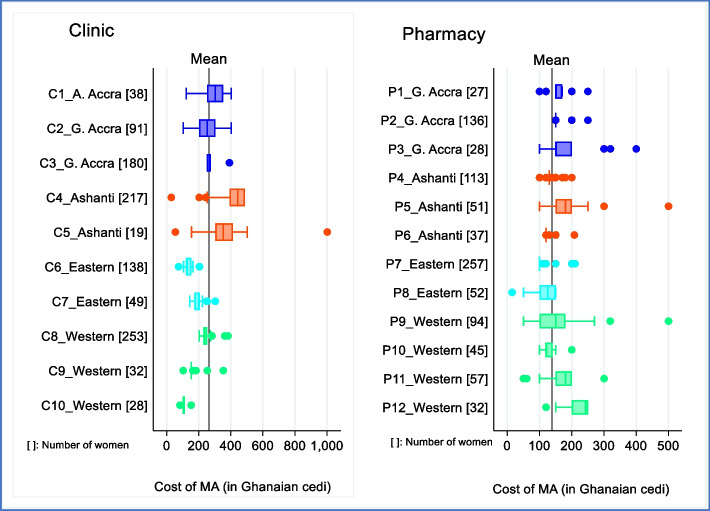
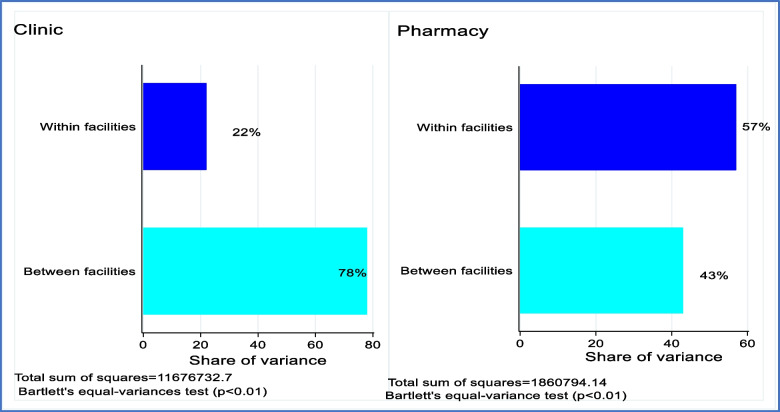
Results: The average costs of MA were approximately US$ 46.00 and US$ 24.00 for the clinic and pharmacy groups, respectively. Additionally, the cost varied between pharmacy and clinic groups and within each group. A greater segment of the variation among the clinic group stemmed from between facilities (78 percent), whereas, among the pharmacies, the bigger share came from within facilities (57 percent). Regression results further indicate that the cost of MA increased among women with higher education, those who have not been in a union with a partner and those who accessed MA in clinics.
Conclusions: MA cost in Ghana is largely based on providers' discretion and at the facility's management level. Additionally, the cost differs by women's socio-demographic attributes. To reduce the disparities in MA costs, developing guidelines to address the health system challenges regarding MA provision and access is important. Educational programs on MA access, provision and legal framework could also reduce abortion-related stigma and cost variations.
Keywords: Healthcare disparities; Medication abortion; Price discrimination; Socio-demographic; Stigmatization.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Approvals from the Ghana Health Service Ethics Review Committee (GHS-ERC012/07/19), University of Ghana Ethics Committee for the Humanities (ECH 034/19–20) and Marie Stopes International Ethics Review Committee (025–19) were obtained for the MOC-Ghana study. Before women were recruited to participate in the MOC-Ghana study, written consent was obtained from them. The Participant Information Sheet (translated into various Ghanaian languages), which contained detailed information about the study, including the potential risks and benefits of participating in the study, was given to each woman to read before providing consent to be interviewed. For those who could not read, the information sheet was read to them in their preferred language. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Pathways to care: Factors predicting women's access to clinic versus pharmacy-based medication abortion in Ghana.Womens Health (Lond). 2025 Jan-Dec;21:17455057251347032. doi: 10.1177/17455057251347032. Epub 2025 Jun 17. Womens Health (Lond). 2025. PMID: 40525558 Free PMC article.
-
Methods for managing miscarriage: a network meta-analysis.Cochrane Database Syst Rev. 2021 Jun 1;6(6):CD012602. doi: 10.1002/14651858.CD012602.pub2. Cochrane Database Syst Rev. 2021. PMID: 34061352 Free PMC article.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Addressing Inequalities in Long Covid Healthcare: A Mixed-Methods Study on Building Inclusive Services.Health Expect. 2025 Aug;28(4):e70336. doi: 10.1111/hex.70336. Health Expect. 2025. PMID: 40600494 Free PMC article.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
Cited by
-
Pathways to care: Factors predicting women's access to clinic versus pharmacy-based medication abortion in Ghana.Womens Health (Lond). 2025 Jan-Dec;21:17455057251347032. doi: 10.1177/17455057251347032. Epub 2025 Jun 17. Womens Health (Lond). 2025. PMID: 40525558 Free PMC article.
References
-
- Bearak J, Popinchalk A, Ganatra B, Moller AB, Tunçalp Ö, Beavin C, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. 2020 Sep 1;8(9):e1152–61. 10.1016/S2214-109X(20)30315-6. - PubMed
-
- Kapp N, Lohr PA. Modern methods to induce abortion: Safety, efficacy and choice. Vol. 63, Best Practice and Research: Clinical Obstetrics and Gynaecology. Bailliere Tindall Ltd; 2020. p. 37–44. 10.1016/j.bpobgyn.2019.11.008. - PubMed
-
- Bankole A, Remez L, Owolabi O, Philbin J, Williams P. From Unsafe to Safe Abortion in Sub-Saharan Africa: Slow but Steady Progress. 2020Dec. 10.1363/2020.32446.
-
- Conti J, Cahill EP. Self-managed abortion. Vol. 31, Current Opinion in Obstetrics and Gynecology. Lippincott Williams and Wilkins; 2019. p. 435–40. 10.1097/GCO.0000000000000585. - PubMed
-
- WHO. Abortion care guideline. 2022. Available from: https://www.who.int/publications/i/item/9789240039483. Cited 2022 Oct 14
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
