

A case of simultaneous adrenalectomy and dissection repair with direct sheath placement into the aorta and systematic review of cases with hyperaldosteronism and vascular dissection: a case report
- PMID: 40390068
- PMCID: PMC12090391
- DOI: 10.1186/s13256-025-05276-1
A case of simultaneous adrenalectomy and dissection repair with direct sheath placement into the aorta and systematic review of cases with hyperaldosteronism and vascular dissection: a case report
Abstract
Background: The incidence of acute aortic dissections is 3-6 patients per 100,000 in a year, with a high mortality rate of 40% at the initial diagnosis and increasing to 90% in an hour. There are several known risk factors for acute aortic dissection; however, the most common risk factor is systemic hypertension. Different conditions have been reported to be associated with resistant hypertension, including hyperaldosteronism.
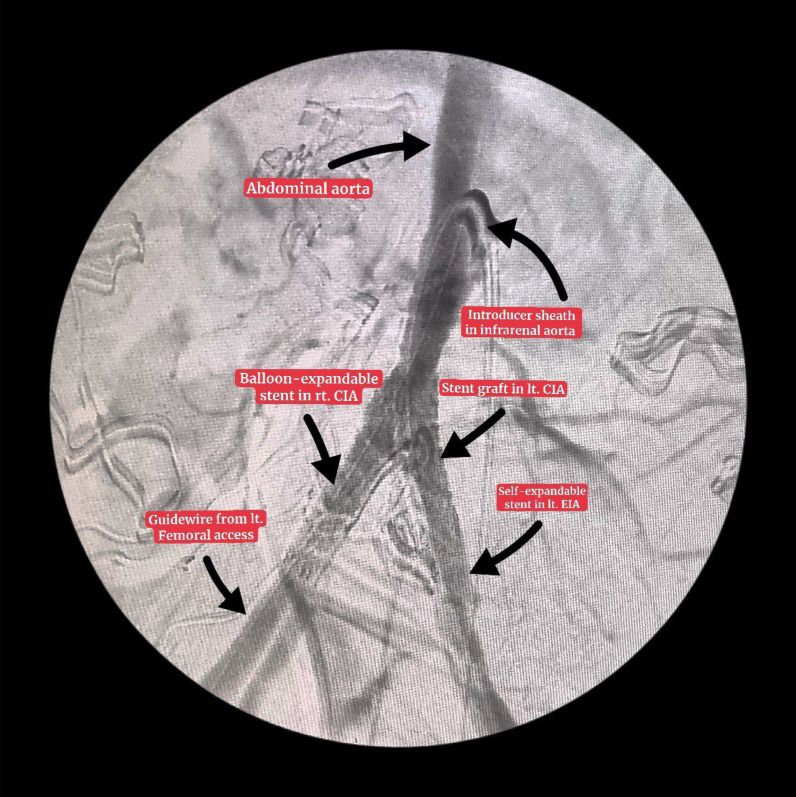
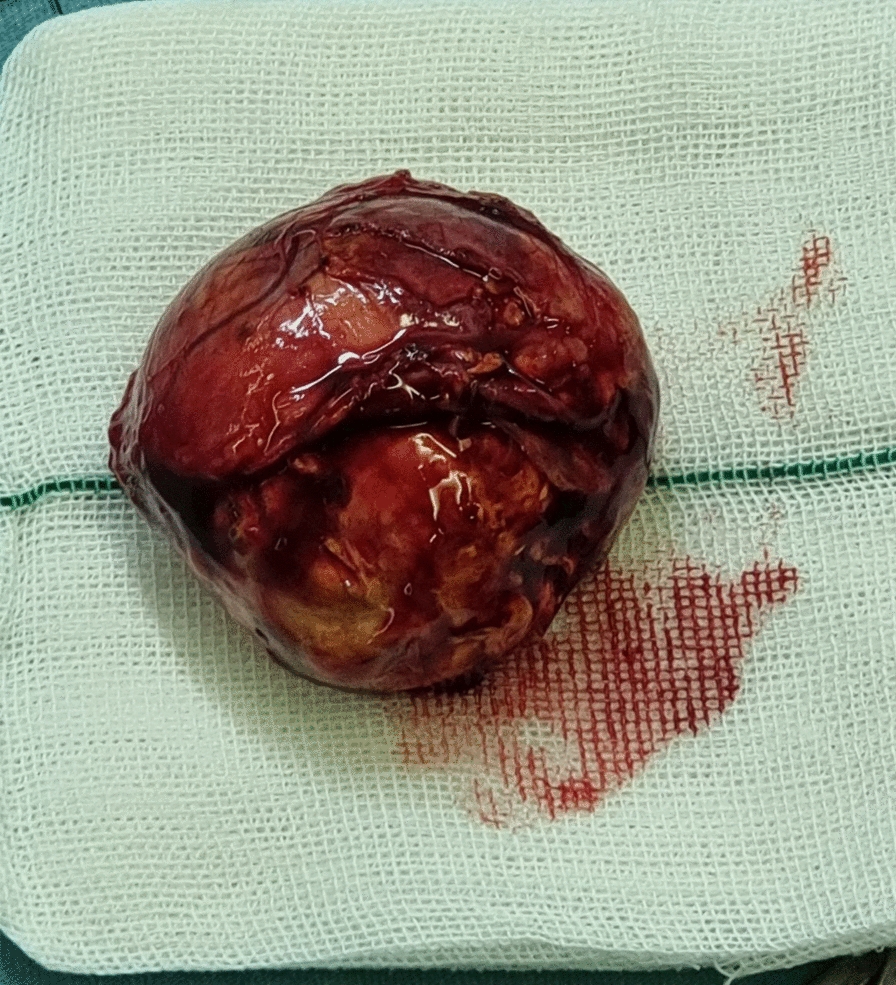
Case presentation: A 57-year-old Persian man came to our clinic with occasional claudication after 30 m distance walking, left leg pain, and symptoms of chronic limb ischemia, including a cold left leg with a shiny appearance. He had a past medical history of recently diagnosed resistant hypertension and a past surgical history of a femoropopliteal bypass and a balloon angioplasty. His computed tomography angiography of the abdominopelvic cavity and lower limbs revealed a dissection of the infrarenal aorta at the bifurcation of common iliac arteries, occlusion of the left external iliac artery, and dissection of the left common iliac artery. In addition, a mass measuring 6 cm × 5 cm × 2 cm was identified in the patient's left adrenal gland. The ostium of the false lumen was in the distal part of dissection so we decided to use an antegrade approach to repair the dissection. He underwent simultaneous surgeries for aneurysmal repair and adrenalectomy.
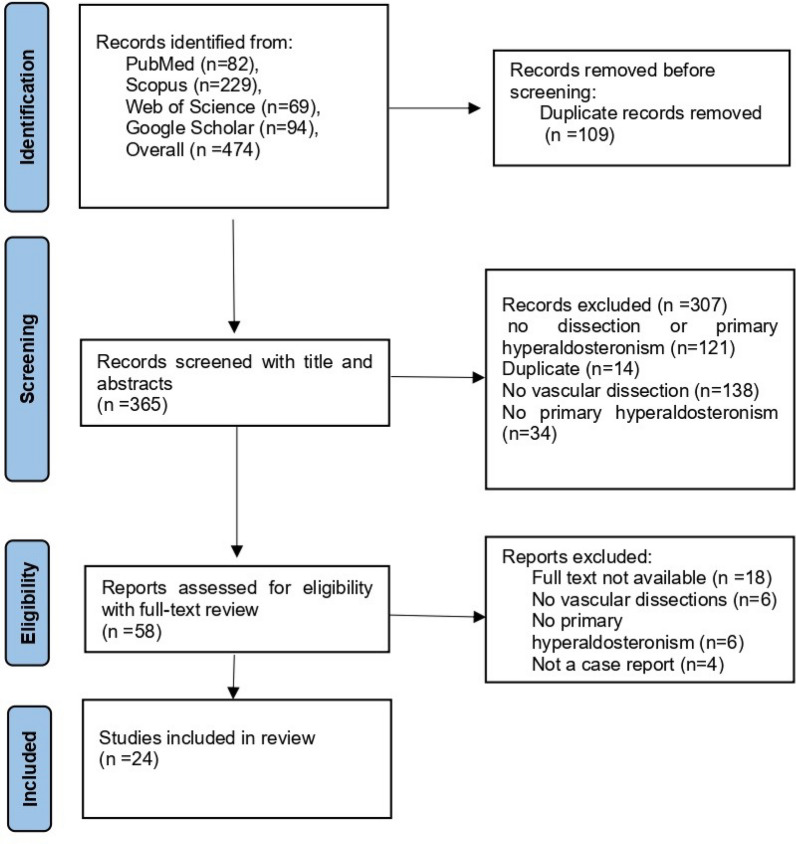
Conclusion: A vast systematic search of literature in Scopus, Web of Science, PubMed, and Google Scholar was carried out to identify cases of hyperaldosteronism relating to vascular dissection that were either treated with surgery or medication. Our results support the theory suggesting that hyperaldosteronism can be considered a risk factor for vascular dissection despite its effects on hypertension.
Keywords: Adrenal glands; Aortic dissection; Blood vessels; Dissection; Hyperaldosteronism.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The patient signed a written informed consent. Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Competing interests: The authors declare that they have no competing interests.
Figures
References
-
- Howard D. Extra-coronary arterial disease: incidence, projected future burden, risk factors and prevention. UK: Oxford University; 2013.
-
- DA C. American Heart Association Professional Education Committee. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Circulation. 2008;117:e510–e26. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
