

Protein disulphide isomerase A4 as a potential biomarker for coronavirus disease 2019: Correlation with cytokine profiles and disease progression
- PMID: 40391685
- PMCID: PMC12118414
- DOI: 10.1080/21505594.2025.2508815
Protein disulphide isomerase A4 as a potential biomarker for coronavirus disease 2019: Correlation with cytokine profiles and disease progression
Abstract
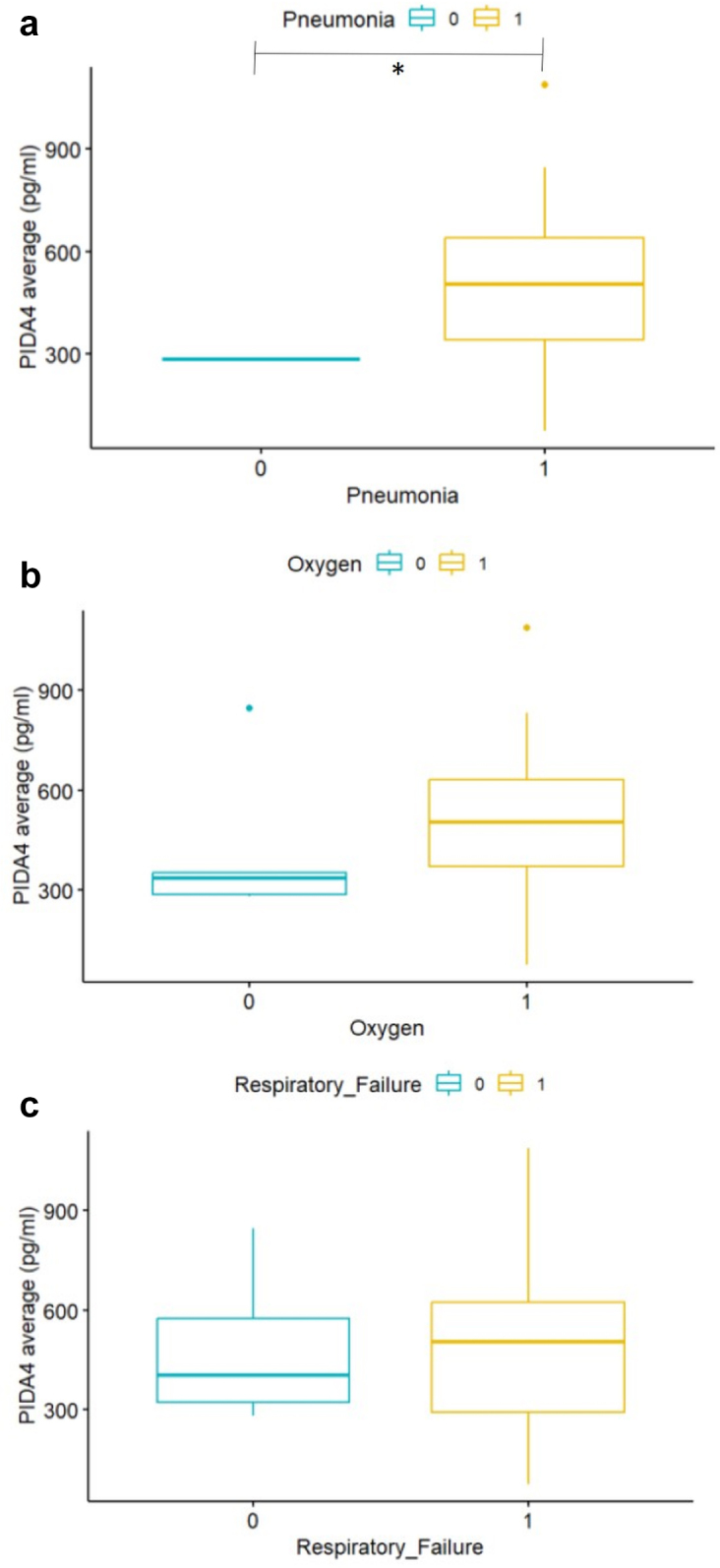
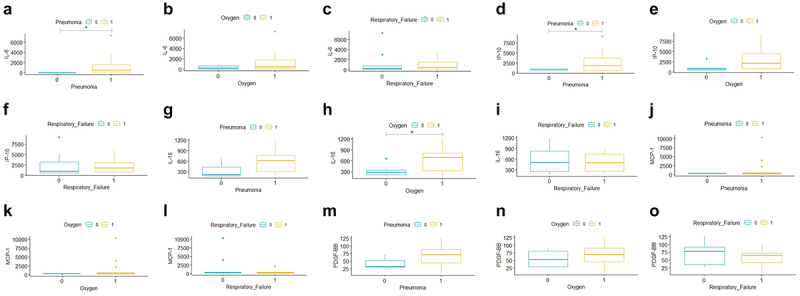
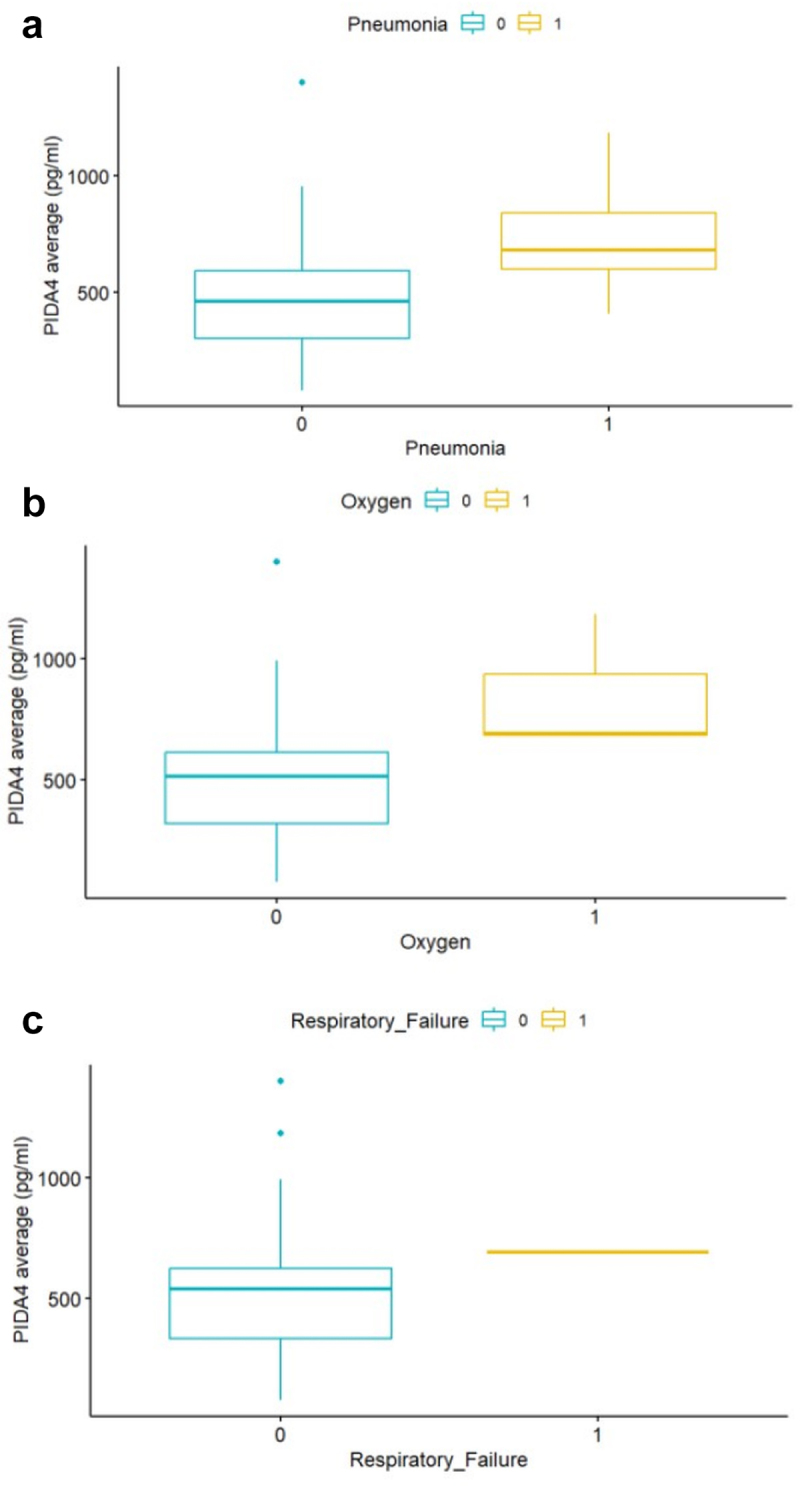
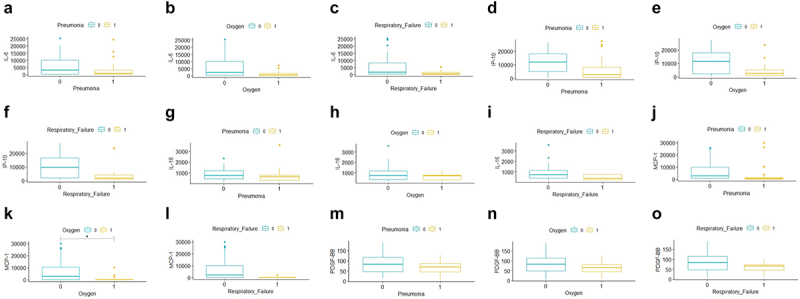
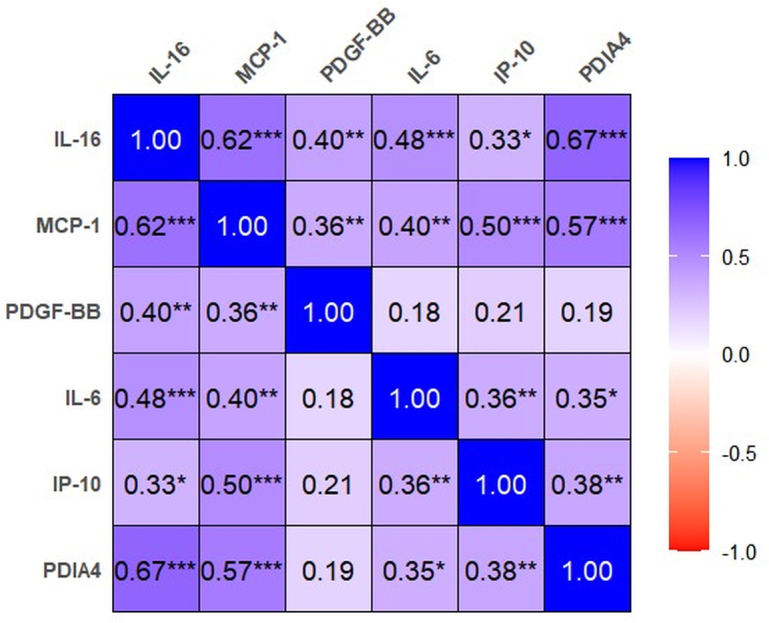
This study investigated the role of protein disulphide isomerase A4 (PDIA4) in the pathogenesis of coronavirus disease 2019 (COVID-19), focusing on its relationship with disease severity and potential as a biomarker. We analysed a cohort of adult COVID-19 patients with varying disease severity, grouped by vaccination status. Serum levels of PDIA4 and cytokines (interleukin [IL]-6, interferon gamma inducible protein-10 [IP-10], IL-16, monocyte chemoattractant protein-1 [MCP-1], and platelet-derived growth factor-BB [PDGF-BB]) were measured using enzyme-linked immunosorbent assay and compared among patients with different disease severities. Statistical analyses were performed to assess the correlation between PDIA4 levels, disease severity, and inflammatory markers. Unvaccinated COVID-19 patients with pneumonia had significantly higher PDIA4 levels than those without pneumonia (517.94 ± 264 vs. 284.86 ± 2.24; p = 0.0022). Although unvaccinated patients requiring oxygen support exhibited higher PDIA4 levels than those not requiring oxygen (519.30 ± 269.67 vs. 420.89 ± 240.49; p = 0.4825), the difference was not statistically significant. No significant difference was observed in the PDIA4 levels between unvaccinated patients with and without respiratory failure. Levels of PDIA4 were positively correlated with the levels of IL-16, MCP-1, IP-10, and IL-6 (correlation coefficients: 0.28-0.62), although this correlation was weaker or absent in vaccinated patients. Our findings suggest that PDIA4 is associated with COVID-19 severity and may serve as a potential biomarker of disease progression. Further studies are needed to elucidate the mechanisms by which PDIA4 influences the immune response and assess its potential for therapeutic exploration in COVID-19.
Keywords: COVID-19; PDIA4; biomarker; cytokines; disease severity.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Hauswald M, BiPAP B, Whittle JS, et al. ACEP COVID-19 Field Guide. 2nd ed. Irving (TX): American College of Emergency Physicians; 2023. Available from: https://www.acep.org/corona/covid-19-field-guide/cover-page
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous