

A New Nomogram for Predicting Early Weight Loss Outcomes in Patients with Obesity Following Laparoscopic Sleeve Gastrectomy
- PMID: 40392476
- PMCID: PMC12270974
- DOI: 10.1007/s11695-025-07798-5
A New Nomogram for Predicting Early Weight Loss Outcomes in Patients with Obesity Following Laparoscopic Sleeve Gastrectomy
Abstract
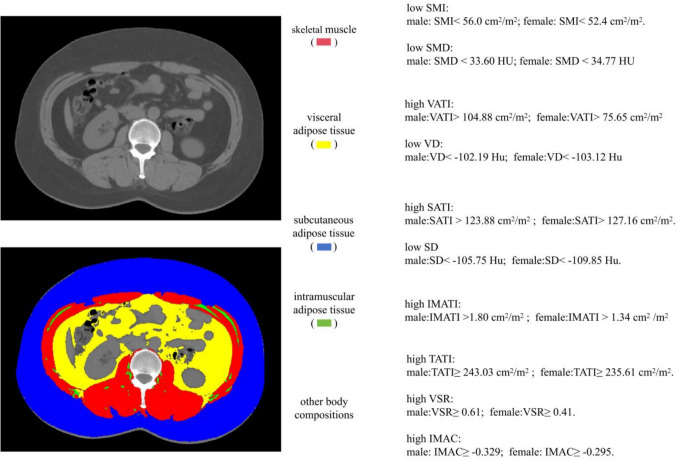
Purpose: Laparoscopic sleeve gastrectomy (LSG) is an effective treatment for obesity, but early weight loss outcomes vary owing to individual nutritional and metabolic differences. We developed a nomogram model to predict early weight loss after LSG, incorporating computed tomography (CT)-based body composition metrics and preoperative inflammatory-nutritional markers.
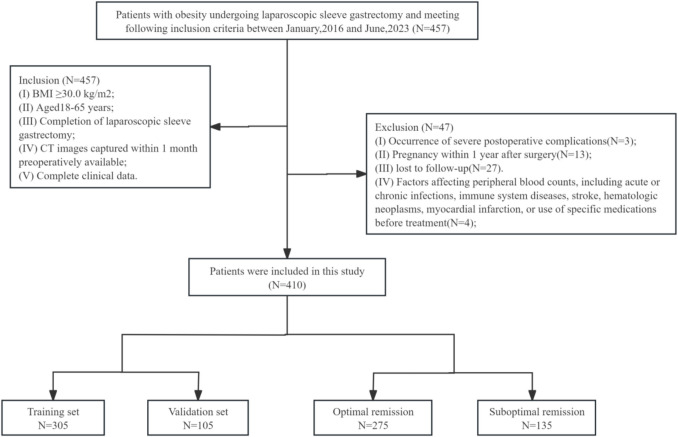
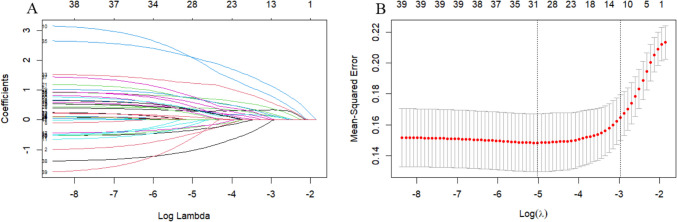
Methods: We retrospectively analyzed 305 patients with obesity who underwent LSG at the Affiliated Hospital of Qingdao University between January 2016 and June 2023. An external validation cohort of 105 patients from a separate institution was also included. Patients were categorized into optimal remission (%total weight loss [%TWL] ≥ 25%) and suboptimal remission (%TWL < 25%) weight loss groups one year postoperatively. Predictive variables were identified using Least Absolute Shrinkage and Selection Operator (LASSO) regression and multivariate logistic regression. A nomogram was constructed based on the significant predictors. Model performance was assessed using the area under the receiver operating characteristic curve (AUC), calibration curves, decision curve analysis (DCA), and clinical impact curve (CIC).
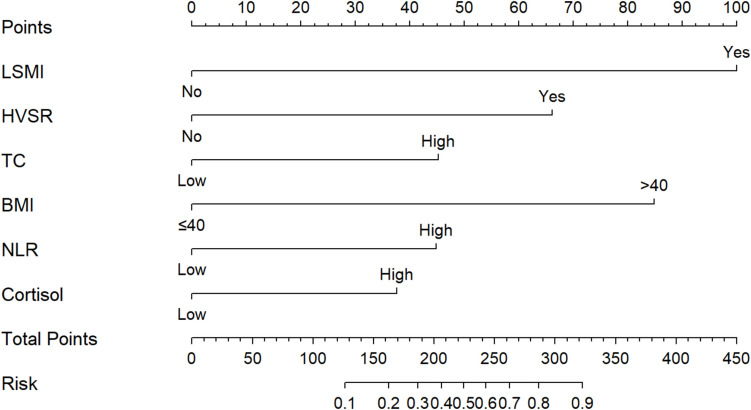
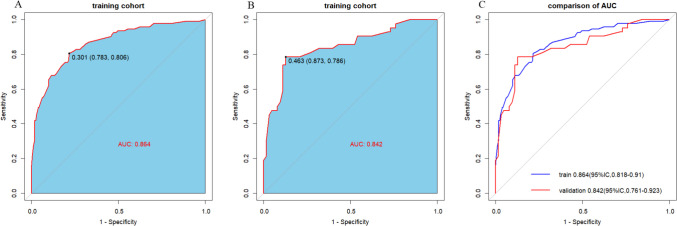
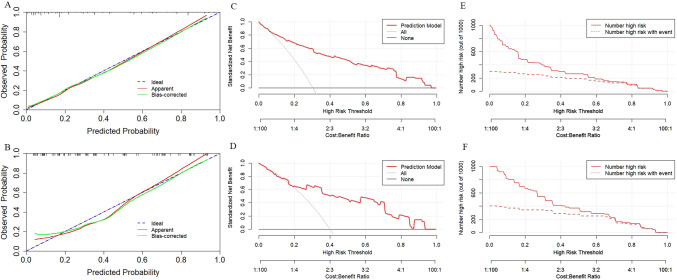
Results: Independent predictors of suboptimal remission included BMI > 40 kg/m2, elevated total cholesterol, high neutrophil-to-lymphocyte ratio, high cortisol, low skeletal muscle index, and elevated visceral-to-subcutaneous adipose tissue area ratio. The constructed nomogram demonstrated strong predictive performance, with AUCs of 0.864 and 0.842 in the training and external validation cohorts, respectively. Calibration curves indicated excellent agreement between predicted and observed outcomes. DCA and CIC confirmed the model's clinical utility in both cohorts.
Conclusion: The developed nomogram effectively predicts early weight loss outcomes after LSG, supporting targeted perioperative management and personalized nutritional interventions.
Keywords: Body composition; Laparoscopic sleeve gastrectomy; Nomogram; Obesity; Predictors.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical Approval: The 1964 Helsinki Declaration and any updates or similar ethical standards, as well as institutional and/or national research committee ethical standards, were followed in all procedures employed in the research involving human beings. The study protocol was approved by Affiliated Hospital of Qingdao University’s ethics committee (approval number, QYFYWZLL28855). Patient Consent Statement: This study was a retrospective study and informed consent was not required. Conflict of Interest: The authors declare no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
