

Chronic Obstructive Pulmonary Disease (COPD): Developments in Pharmacological Treatments
- PMID: 40392521
- PMCID: PMC12185658
- DOI: 10.1007/s40265-025-02188-8
Chronic Obstructive Pulmonary Disease (COPD): Developments in Pharmacological Treatments
Abstract
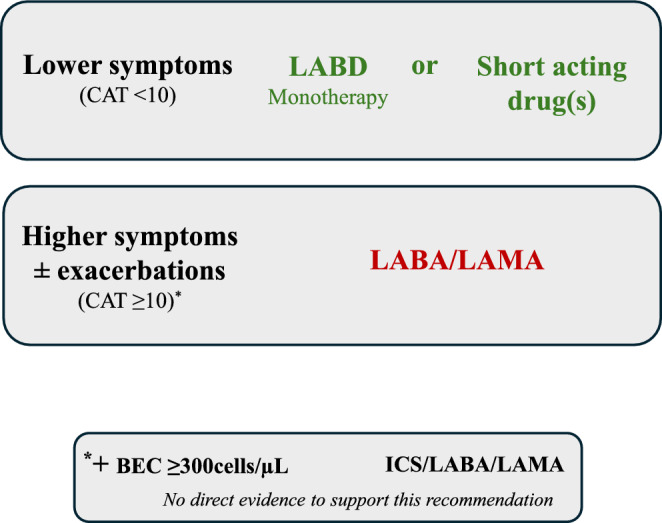
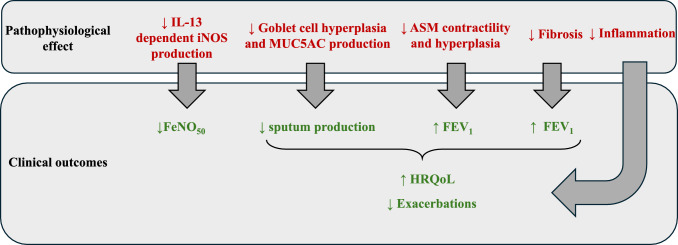
The immediate goals of pharmacological management in chronic obstructive pulmonary disease (COPD) are to minimise symptoms and improve exercise performance. The longer-term goals are to reduce the future risk of exacerbations, lung function decline and mortality. It is now recognised that a subset of COPD patients have type 2 inflammation, which is identified by the presence of higher blood eosinophil counts (BEC). Individuals with higher BEC show a greater response to pharmacological interventions targeting type 2 inflammation, including inhaled corticosteroids and the monoclonal antibody, dupilumab. The use of BEC as a biomarker to guide pharmacological treatment has enabled a precision medicine approach in COPD. This article reviews recent advances in the pharmacological treatment of COPD, encompassing the optimum use of inhaled combination treatments and the evidence to support the use of the novel inhaled phosphodiesterase inhibitor ensifentrine and monoclonal antibodies in patients with COPD.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Funding: The authors did not receive any funding for this paper. Conflict of interest: DS has received personal fees from Adovate, Aerogen, Almirall, Apogee, Arrowhead, AstraZeneca, Bial, Boehringer Ingelheim, Chiesi, Cipla, CONNECT Biopharm, Covis, CSL Behring, DevPro Biopharma LCC, Elpen, Empirico, EpiEndo, Genentech, Generate Biomedicines, GlaxoSmithKline, Glenmark, Kamada, Kinaset Therapeutics, Kymera, Menarini, MicroA, OM Pharma, Orion, Pieris Pharmaceuticals, Pulmatrix, Revolo, Roivant Sciences, Sanofi, Synairgen, Tetherex, Teva, Theravance Biopharma, Upstream and Verona Pharma. AGM has received honoraria from GlaxoSmithKline and Sanofi and has received non-financial support from Verona pharma, all not related to this work. AH has received honoraria for lecturing from Chiesi. AB has no conflicts to declare. Availability of data: Not applicable. Ethics approval: Not applicable. Consent to participate: Not applicable. Consent for publication: Not applicable. Code availability: Not applicable. Author contributions: DS, AH, AM and AB contributed to writing and reviewing the manuscript. All authors read and approved the final manuscript.
Figures



References
-
- Collaborators GCoD. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2100–32. 10.1016/s0140-6736(24)00367-2. - PMC - PubMed
-
- Collaborators GCoD. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2133–61.10.1016/s0140-6736(24)00757-8. - PMC - PubMed
-
- Sin DD, Ron D, Agusti A, et al. Air pollution and COPD: GOLD 2023 committee report. Eur Respir J. 2023. 10.1183/13993003.02469-2022. - PubMed
-
- Lange P, Celli B, Agustí A, et al. Lung-function trajectories leading to chronic obstructive pulmonary disease. N Engl J Med. 2015;373(2):111–22. 10.1056/NEJMoa1411532. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
