

Early Prediction of Mortality Risk in Acute Respiratory Distress Syndrome: Systematic Review and Meta-Analysis
- PMID: 40392588
- PMCID: PMC12134695
- DOI: 10.2196/70537
Early Prediction of Mortality Risk in Acute Respiratory Distress Syndrome: Systematic Review and Meta-Analysis
Abstract
Background: Acute respiratory distress syndrome (ARDS) is a life-threatening condition associated with high mortality rates. Despite advancements in critical care, reliable early prediction methods for ARDS-related mortality remain elusive. Accurate risk assessment is crucial for timely intervention and improved patient outcomes. Machine learning (ML) techniques have emerged as promising tools for mortality prediction in patients with ARDS, leveraging complex clinical datasets to identify key prognostic factors. However, the efficacy of ML-based models remains uncertain. This systematic review aims to assess the value of ML models in the early prediction of ARDS mortality risk and to provide evidence supporting the development of simplified, clinically applicable ML-based scoring tools for prognosis.
Objective: This study systematically reviewed available literature on ML-based ARDS mortality prediction models, primarily aiming to evaluate the predictive performance of these models and compare their efficacy with conventional scoring systems. It also sought to identify limitations and provide insights for improving future ML-based prediction tools.
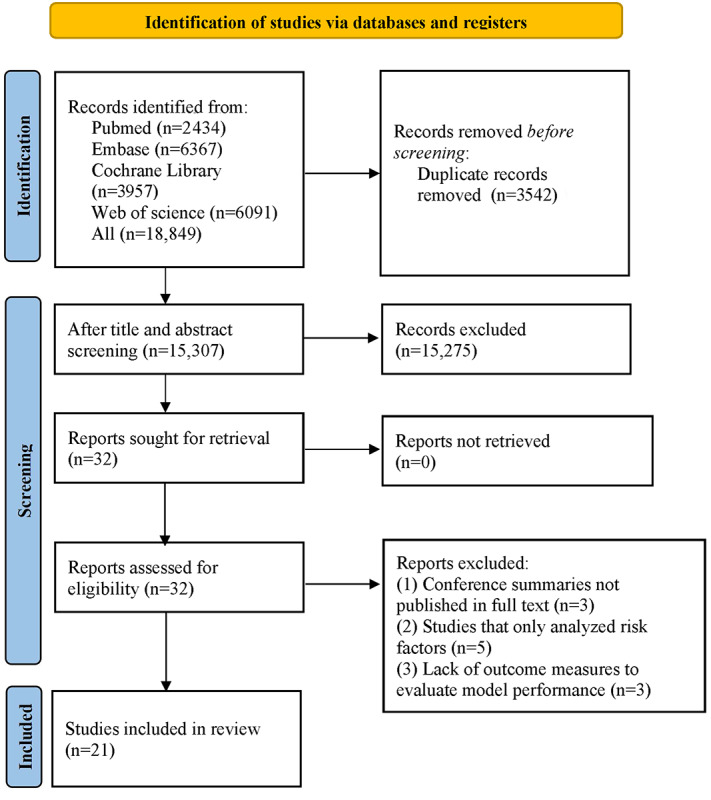
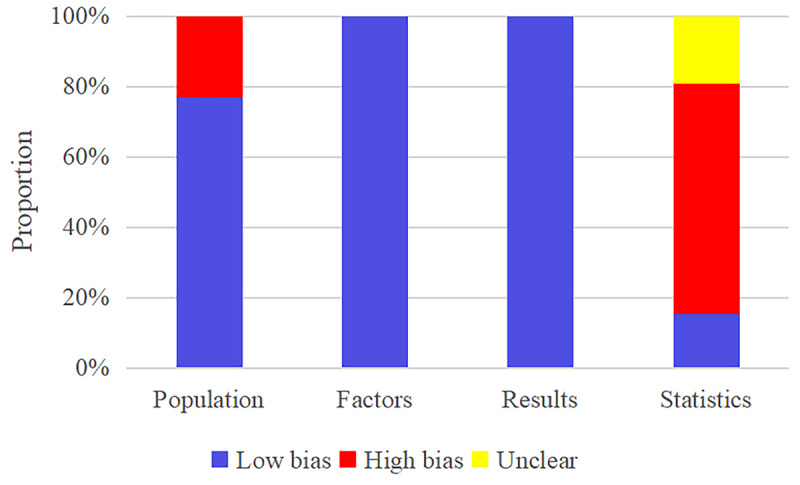
Methods: A comprehensive literature search was conducted across PubMed, Web of Science, the Cochrane Library, and Embase, covering publications from inception to April 27, 2024. Studies developing or validating ML-based ARDS mortality predicting models were considered for inclusion. The methodological quality and risk of bias were assessed using the Prediction Model Risk of Bias Assessment Tool (PROBAST). Subgroup analyses were performed to explore heterogeneity in model performance based on dataset characteristics and validation approaches.
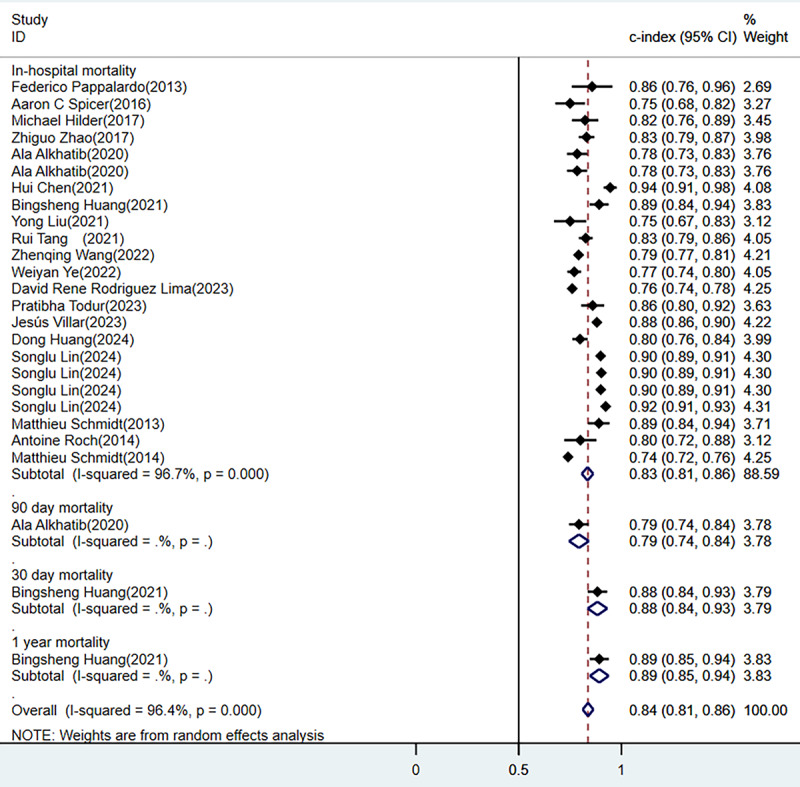
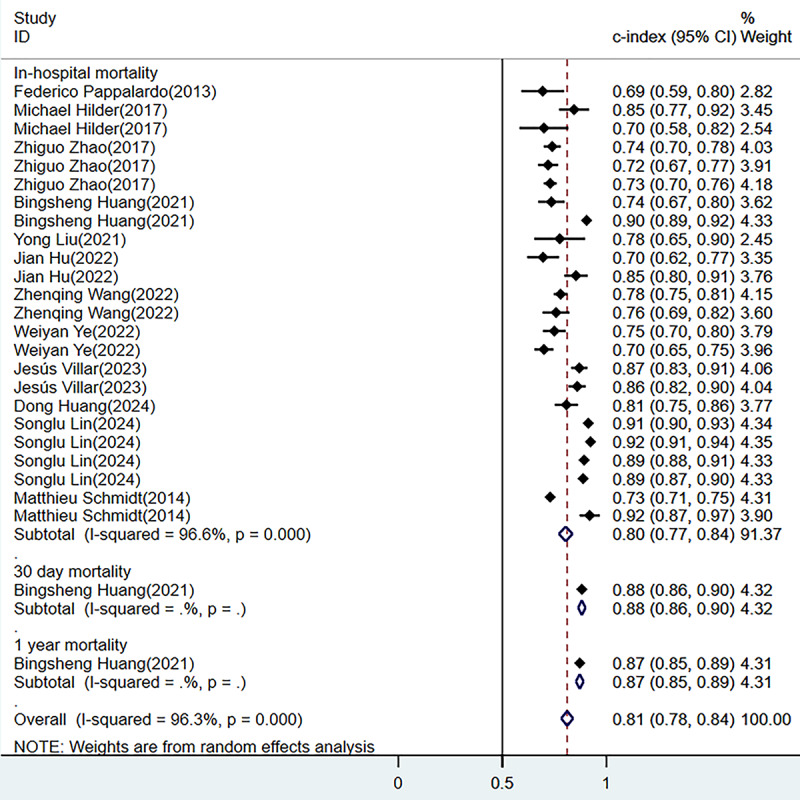
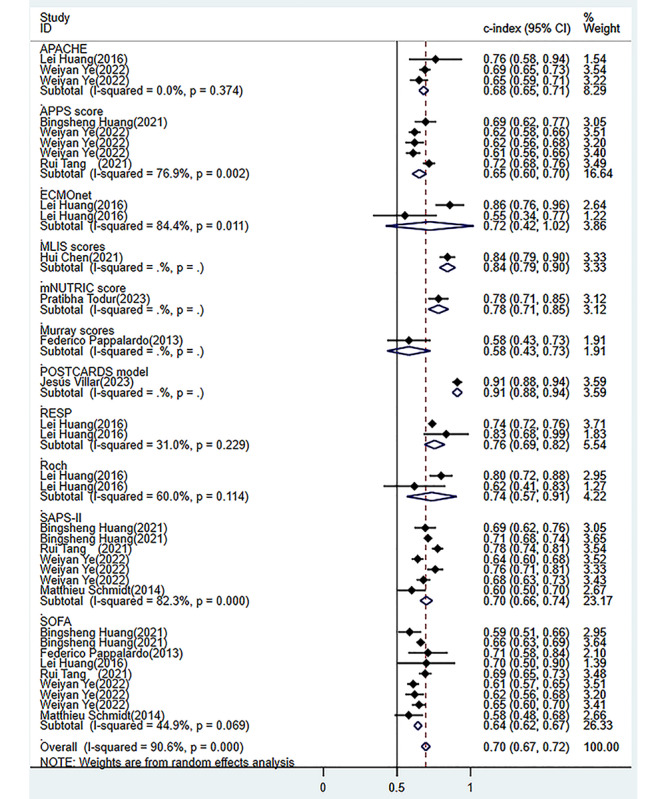
Results: In total, 21 studies involving a total of 31,291 patients with ARDS were included. The meta-analysis demonstrated that ML models achieved relatively high predictive performance. In the training datasets, the pooled concordance index (C-index) was 0.84 (95% CI 0.81-0.86), while for in-hospital mortality prediction, the pooled C-index was 0.83 (95% CI 0.81-0.86). In the external validation datasets, the pooled C-index was 0.81 (95% CI 0.78-0.84), and the corresponding value for in-hospital mortality prediction was 0.80 (95% CI 0.77-0.84). ML models outperformed traditional scoring tools, which demonstrated lower predictive performance. The pooled area under the receiver operating characteristic curve (ROC-AUC) for standard scoring systems was 0.7 (95% CI 0.67-0.72). Specifically, 2 widely used clinical scoring systems, the Sequential Organ Failure Assessment (SOFA) and Simplified Acute Physiology Score II (SAPS-II), demonstrated ROC-AUCs of 0.64 (95% CI 0.62-0.67) and 0.70 (95% CI 0.66-0.74), respectively.
Conclusions: ML-based models exhibited superior predictive accuracy over conventional scoring tools, suggesting their potential use in early ARDS mortality risk assessment. However, further research is needed to refine these models, improve their interpretability, and enhance their clinical applicability. Future efforts should focus on developing simplified, efficient, and user-friendly ML-based prediction tools that integrate seamlessly into clinical workflows. Such advancements may facilitate the early identification of high-risk patients, enabling timely interventions and personalized, risk-based prevention strategies to improve ARDS outcomes.
Keywords: acute respiratory distress syndrome; machine learning; meta-analysis; mortality; systematic review.
©Ruimin Tan, Chen Ge, Zhe Li, Yating Yan, He Guo, Wenjing Song, Qiong Zhu, Quansheng Du. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 20.05.2025.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Predictive Modeling of Acute Respiratory Distress Syndrome Using Machine Learning: Systematic Review and Meta-Analysis.J Med Internet Res. 2025 May 13;27:e66615. doi: 10.2196/66615. J Med Internet Res. 2025. PMID: 40359510 Free PMC article.
-
Mortality prediction for patients with acute respiratory distress syndrome based on machine learning: a population-based study.Ann Transl Med. 2021 May;9(9):794. doi: 10.21037/atm-20-6624. Ann Transl Med. 2021. PMID: 34268407 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Machine learning-based risk predictive models for diabetic kidney disease in type 2 diabetes mellitus patients: a systematic review and meta-analysis.Front Endocrinol (Lausanne). 2025 Mar 3;16:1495306. doi: 10.3389/fendo.2025.1495306. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40099258 Free PMC article.
-
Evaluation of machine learning methods for prediction of heart failure mortality and readmission: meta-analysis.BMC Cardiovasc Disord. 2025 Apr 7;25(1):264. doi: 10.1186/s12872-025-04700-0. BMC Cardiovasc Disord. 2025. PMID: 40189534 Free PMC article.
Cited by
-
Artificial intelligence and machine learning in acute respiratory distress syndrome management: recent advances.Front Med (Lausanne). 2025 Jul 16;12:1597556. doi: 10.3389/fmed.2025.1597556. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40740956 Free PMC article. Review.
References
-
- dos Santos CC, Slutsky AS. Protective ventilation of patients with acute respiratory distress syndrome. Crit Care. 2004;8(3):145–147. doi: 10.1186/cc2849. https://ccforum.biomedcentral.com/articles/10.1186/cc2849 cc2849 - DOI - DOI - PMC - PubMed
-
- Matthay MA, Arabi Y, Arroliga AC, Bernard G, Bersten AD, Brochard LJ, Calfee CS, Combes A, Daniel BM, Ferguson ND, Gong MN, Gotts JE, Herridge MS, Laffey JG, Liu KD, Machado FR, Martin TR, McAuley DF, Mercat A, Moss M, Mularski RA, Pesenti A, Qiu H, Ramakrishnan N, Ranieri VM, Riviello ED, Rubin E, Slutsky AS, Thompson BT, Twagirumugabe T, Ware LB, Wick KD. A new global definition of acute respiratory distress syndrome. Am J Respir Crit Care Med. 2024;209(1):37–47. doi: 10.1164/rccm.202303-0558WS. https://europepmc.org/abstract/MED/37487152 - DOI - PMC - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A, LUNG SAFE Investigators. ESICM Trials Group Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. doi: 10.1001/jama.2016.0291.2492877 - DOI - PubMed
-
- Liu L, Yang Y, Gao Z, Li M, Mu X, Ma X, Li G, Sun W, Wang X, Gu Q, Zheng R, Zhao H, Ao D, Yu W, Wang Y, Chen K, Yan J, Li J, Cai G, Wang Y, Wang H, Kang Y, Slutsky AS, Liu S, Xie J, Qiu H. Practice of diagnosis and management of acute respiratory distress syndrome in mainland China: a cross-sectional study. J Thorac Dis. 2018;10(9):5394–5404. doi: 10.21037/jtd.2018.08.137. https://europepmc.org/abstract/MED/30416787 jtd-10-09-5394 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
