

Endoscopic Vacuum Therapy for Anastomotic Leakage After Distal Gastrectomy in a Renal Transplant Patient: A Case Study
- PMID: 40392762
- PMCID: PMC12103060
- DOI: 10.12659/AJCR.946626
Endoscopic Vacuum Therapy for Anastomotic Leakage After Distal Gastrectomy in a Renal Transplant Patient: A Case Study
Abstract
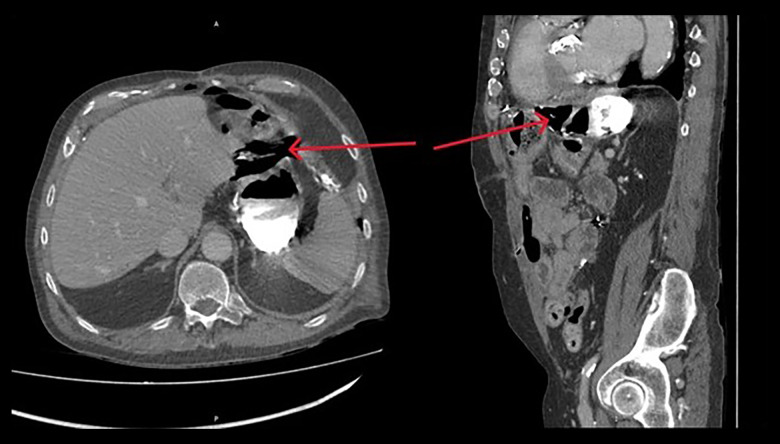
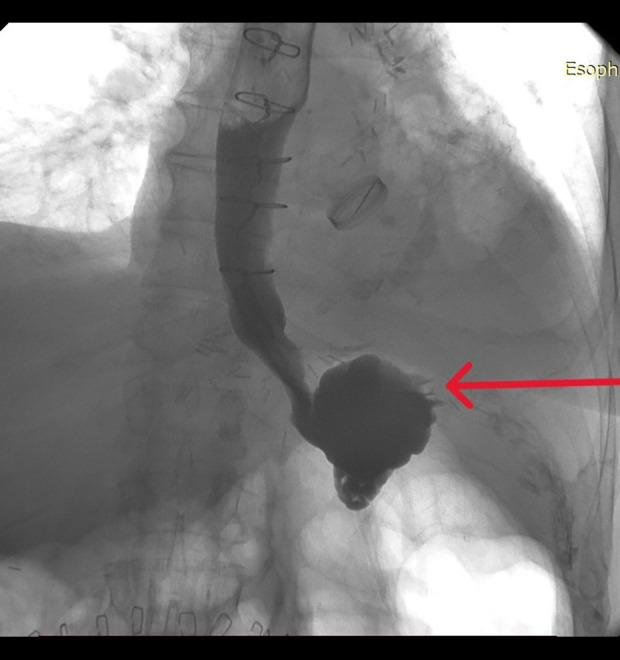
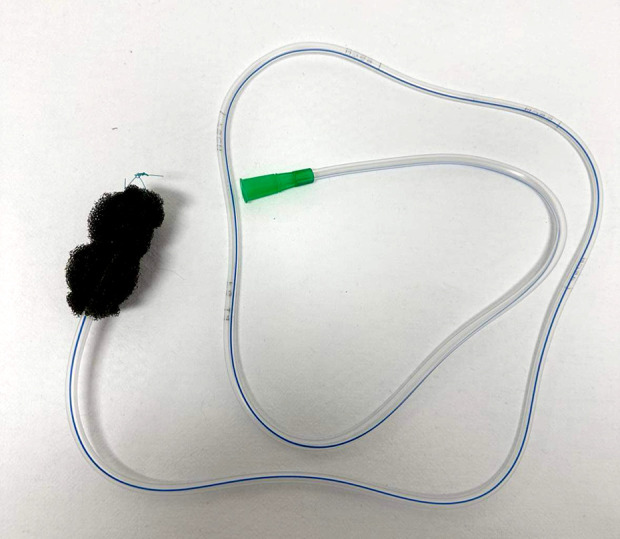
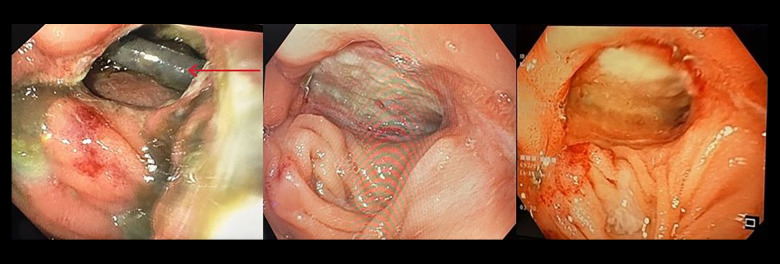
BACKGROUND Since the late 2000's, endoscopic vacuum therapy (EVT) has gained popularity in the management of anastomotic leakage (AL) of the upper gastrointestinal (GI) tract due to its safety and efficacy. This report describes a 66-year-old male renal transplant patient with an AL following distal gastrectomy for gastric adenocarcinoma and was treated with EVT. CASE REPORT We present the case of a 66-year-old transplant patient with multiple comorbidities who developed AL following distal gastrectomy for gastric adenocarcinoma. Before the scheduled operation, he had been deemed at high risk for AL due to immunosuppression, as well as his history of end-stage renal disease and multiple abdominal surgeries. After an initial failed attempt to treat the AL surgically, he became the first person to be treated with a self-assembled EVT in our hospital. He was successfully treated with EVT and was ultimately safely discharged. Also, 30 days after discharge, he did not report any discomfort or express any problems with oral intake of food, as supported by the findings of a follow-up endoscopy. CONCLUSIONS EVT is a reproducible technique, which when performed by experienced practitioners, remains effective even in the absence of prior experience with the procedure or even procedure-specific equipment. The technique shows promising outcomes in the management of AL and this case highlights the technique's effectiveness even in a patient with compromised wound healing in the presence of a hostile abdomen.
Conflict of interest statement
Figures
Similar articles
-
Endoscopic vacuum therapy for anastomotic leakage after upper gastrointestinal surgery.Endoscopy. 2023 Nov;55(11):1019-1025. doi: 10.1055/a-2102-1691. Epub 2023 May 30. Endoscopy. 2023. PMID: 37253387 Free PMC article. Clinical Trial.
-
Self-Expanding Metal Stents Versus Endoscopic Vacuum Therapy in Anastomotic Leak Treatment After Oncologic Gastroesophageal Surgery.J Gastrointest Surg. 2019 Jan;23(1):67-75. doi: 10.1007/s11605-018-4000-x. Epub 2018 Oct 29. J Gastrointest Surg. 2019. PMID: 30374816
-
Long-Term Quality of Life Assessment After Successful Endoscopic Vacuum Therapy of Defects in the Upper Gastrointestinal Tract Quality of Life After EVT.J Gastrointest Surg. 2019 Feb;23(2):280-287. doi: 10.1007/s11605-018-4038-9. Epub 2018 Nov 14. J Gastrointest Surg. 2019. PMID: 30430432
-
Systematic review of endoluminal vacuum-assisted therapy as salvage treatment for rectal anastomotic leakage.BJS Open. 2018 Dec 26;3(2):153-160. doi: 10.1002/bjs5.50124. eCollection 2019 Apr. BJS Open. 2018. PMID: 30957061 Free PMC article.
-
Endoscopic vacuum therapy in the upper gastrointestinal tract: when and how to use it.Langenbecks Arch Surg. 2022 May;407(3):957-964. doi: 10.1007/s00423-022-02436-5. Epub 2022 Jan 18. Langenbecks Arch Surg. 2022. PMID: 35041047 Free PMC article. Review.
Cited by
-
VacStent as a novel therapeutic approach for esophageal perforations and anastomotic leaks- a systematic review of the literature.BMC Surg. 2025 Jul 21;25(1):309. doi: 10.1186/s12893-025-03067-5. BMC Surg. 2025. PMID: 40691570 Free PMC article.
References
-
- Turrentine FE, Denlinger CE, Simpson VB, et al. Morbidity, mortality, cost, and survival estimates of gastrointestinal anastomotic leaks. J Am Coll Surg. 2015;220(2):195–206. - PubMed
-
- Eriksen TF, Lassen CB, Gögenur I. Treatment with corticosteroids and the risk of anastomotic leakage following lower gastrointestinal surgery: A literature survey. Colorectal Dis. 2014;16(5):O154–O160. - PubMed
-
- Phillips B. Reducing gastrointestinal anastomotic leak rates: Review of challenges and solutions. Open Access Surg. 2016;9:5–14.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
