

Marshall-Plan Ablation Strategy Versus Pulmonary Vein Isolation in Persistent AF: A Randomized Controlled Trial
- PMID: 40392905
- PMCID: PMC12094258
- DOI: 10.1161/CIRCEP.124.013427
Marshall-Plan Ablation Strategy Versus Pulmonary Vein Isolation in Persistent AF: A Randomized Controlled Trial
Abstract
Background: Beyond pulmonary vein (PV) isolation, the optimal ablation strategy for persistent atrial fibrillation (AF) remains poorly defined. The purpose of this study was to compare 2 ablation strategies in the treatment of patients with persistent AF: a comprehensive ablation strategy based on anatomic considerations versus PV isolation alone.
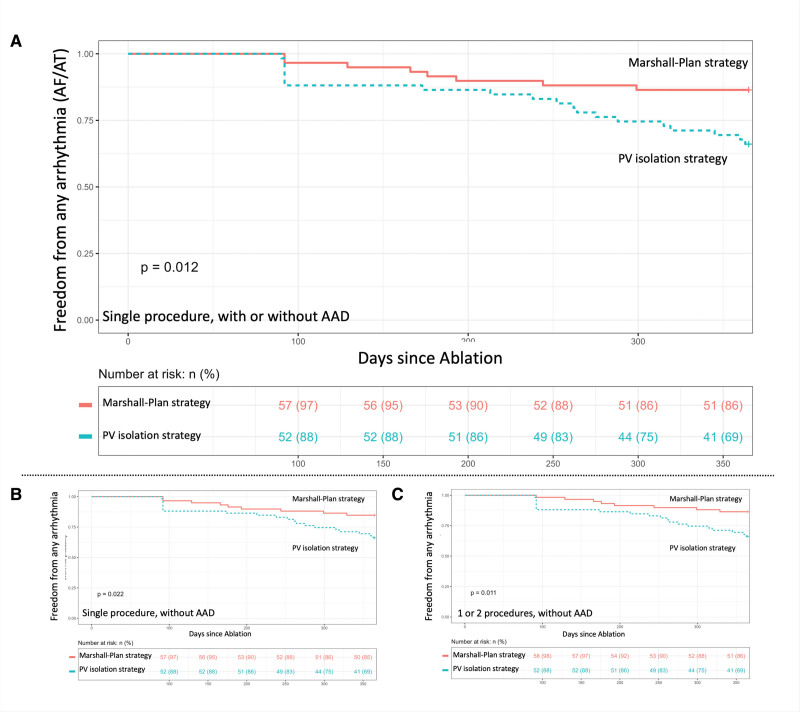
Methods: The Marshall-Plan trial is a prospective, randomized, parallel-group, controlled clinical trial of superiority conducted at the Bordeaux University Hospital. Consecutive patients with symptomatic, documented persistent AF were included and randomized into 2 arms: Marshall-Plan consisting of PV isolation with additional ablation including vein of Marshall ethanol infusion, and lines of block at the mitral, dome, and cavotricuspid isthmuses versus PV isolation alone. The main outcome was the 1-year freedom from any arrhythmia (atrial fibrillation/atrial tachycardia >30 seconds) after a single ablation procedure with or without any antiarrhythmic medication at 12 months.
Results: A total of 120 patients were included (age 65±8 years; 21 women). Two patients were excluded from analysis. All PVs were successfully isolated in both groups. In the Marshall-Plan group, vein of Marshall ethanol infusion was completed in 57 (97%) patients. Conduction block across linear lesions was obtained in 93%, 92%, and 93% of the mitral, dome, and cavotricuspid isthmuses, respectively. The full lesion set was successfully completed in 52 (88%) patients in the Marshall-Plan group and 59 (100%) patients in the PV isolation group. At 12 months, freedom from recurrence of atrial arrhythmia >30 seconds after 1 ablation procedure, with or without antiarrhythmic medication, had occurred in 51 of the 59 (86.4%) patients assigned to the Marshall-Plan approach, and 39 of the 59 (66.1%) patients assigned to PV isolation only (P=0.012).
Conclusions: In this prospective randomized controlled trial, the Marshall-Plan strategy was significantly superior to a PV isolation strategy at 12 months.
Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT04206982.
Keywords: cardiac arrhythmia; ethanol; heart; human; pulmonary veins; tachycardia; therapeutics.
Conflict of interest statement
Dr Derval received modest consulting fees and speaking honoraria from Biosense Webster. Dr Duchateau received modest consulting fees and speaking honoraria from Biosense Webster. Dr Sacher received modest consulting fees and speaking honoraria from Biosense Webster, Boston Scientific, Abbott, Medtronic, and consulting fees from Biosense Webster. Dr Jaïs, received modest consulting fees and speaking honoraria from Biosense Webster, Boston Scientific, Abbott, and Medtronic, and consulting fees from Biosense Webster. Dr Pambrun received modest consulting fees and speaking honoraria from Biosense Webster. The other authors report no conflicts.
Figures



References
-
- Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, Akar JG, Badhwar V, Brugada J, Camm J, et al. . 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14:e275–e444. doi: 10.1016/j.hrthm.2017.05.012 - PMC - PubMed
-
- Derval N, Duchateau J, Denis A, Ramirez FD, Mahida S, André C, Krisai P, Nakatani Y, Kitamura T, Takigawa M, et al. . Marshall bundle elimination, pulmonary vein isolation, and line completion for anatomical ablation of persistent atrial fibrillation (Marshall-PLAN): Prospective, single-center study. Heart Rhythm. 2021;18:529–537. doi: 10.1016/j.hrthm.2020.12.023 - PubMed
-
- Pambrun T, Denis A, Duchateau J, Sacher F, Hocini M, Jaïs P, Haïssaguerre M, Derval N. MARSHALL bundles elimination, pulmonary veins isolation and lines completion for anatomical ablation of persistent atrial fibrillation: MARSHALL-PLAN case series. J Cardiovasc Electrophysiol. 2019;30:7–15. doi: 10.1111/jce.13797 - PubMed
-
- Pambrun T, Derval N, Duchateau J, Denis A, Chauvel R, Tixier R, Welte N, André C, Nakashima T, Nakatani Y, et al. . Epicardial course of the musculature related to the great cardiac vein: anatomical considerations and clinical implications for mitral isthmus block after vein of Marshall ethanol infusion. Heart Rhythm. 2021;18:1951–1958. doi: 10.1016/j.hrthm.2021.06.1202 - PubMed
-
- Pambrun T, Duchateau J, Delgove A, Denis A, Constantin M, Ramirez FD, Chauvel R, Tixier R, Welte N, André C, et al. . Epicardial course of the septopulmonary bundle: anatomical considerations and clinical implications for roof line completion. Heart Rhythm. 2021;18:349–357. doi: 10.1016/j.hrthm.2020.11.008 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
