

Efficacy, Safety, and Cost-Effectiveness of "Internet + Pharmacy Care" Via the Alfalfa App in Warfarin Therapy Management After Cardiac Valve Replacement: Randomized Controlled Trial
- PMID: 40393057
- PMCID: PMC12112255
- DOI: 10.2196/53586
Efficacy, Safety, and Cost-Effectiveness of "Internet + Pharmacy Care" Via the Alfalfa App in Warfarin Therapy Management After Cardiac Valve Replacement: Randomized Controlled Trial
Abstract
Background: Anticoagulation management is important in preventing complications in patients undergoing cardiac valve replacement. The development of mobile apps offers new opportunities for the management of long-term anticoagulants. However, there is a lack of randomized controlled trials evaluating the effectiveness, safety, cost-effectiveness, and user demand for internet-based anticoagulation management.
Objective: This study aimed to evaluate the efficacy, safety, and cost-effectiveness of a 3-month warfarin dose adjustment mobile app Alfalfa compared to offline management in patients postcardiac valve replacement. We also explored the app's feasibility on user satisfaction and demand.
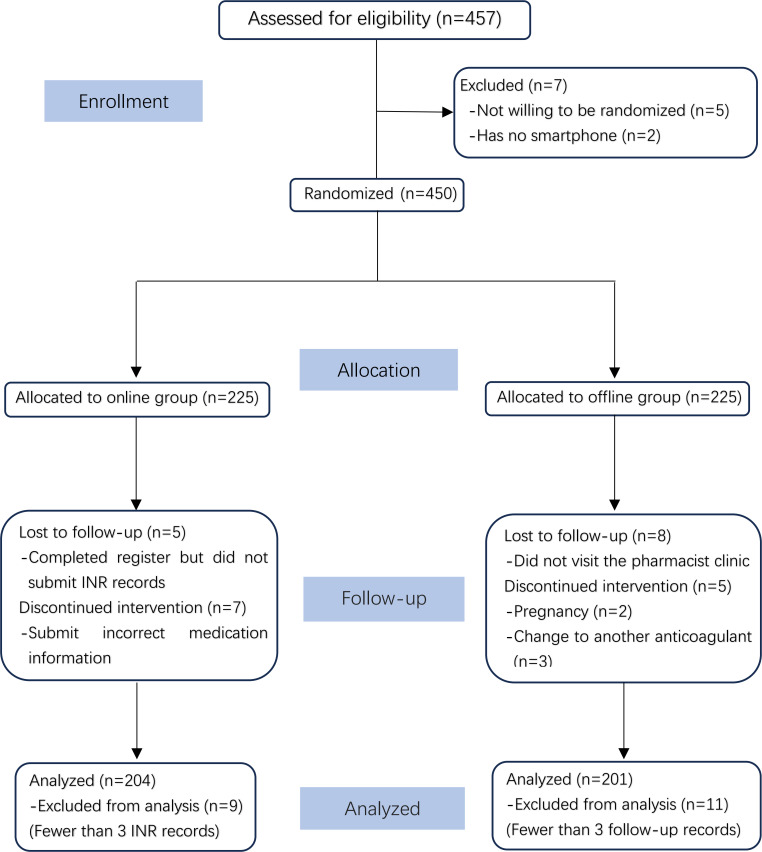
Methods: This study was a randomized controlled trial with assessments conducted at baseline and at a 3-month follow-up. Participants were eligible if they had been on warfarin therapy for at least 3 months, received warfarin management either through the Alfalfa app or through pharmacist-led anticoagulation outpatient clinic visits, consented to regular follow-ups, and had not experienced serious bleeding or thrombotic events in the 3 months before warfarin treatment. A P value of ≤.05 was considered statistically significant.
Results: A total of 405 participants were included in the analysis. The time in therapeutic range was significantly higher in the Alfalfa app group than in the offline group (66.46% vs 46.65%, P<.001). Participants in the Alfalfa app group had a higher monitoring frequency (8.14 vs 4.47, P<.001) and a greater percentage of international normalized ratio values within the target range (896/1660, 53.98% vs 346/899, 38.49%; P<.001) than those in the offline group. In addition, the Alfalfa app group exhibited lower rates of subtherapeutic (235/1660, 14.16% vs 152/899, 16.91%; P<.05) and extreme subtherapeutic international normalized ratio values (273/1660, 16.45% vs 186/899, 20.69%; P<.05) than the offline group. However, the incidence of minor bleeding was higher in the Alfalfa app group (12/204, 5.9% vs 3/201, 1.5%; P=.02). In terms of cost-effectiveness, the Alfalfa app group had a significantly lower average cost per test (42.37 vs 78.3, P<.001), average time per test (47.42 vs 90.74, P<.001), and cost-effectiveness ratio (385.9 vs 662.9) than the offline group. A total of 86 participants completed the satisfaction questionnaire, and the vast majority of participants expressed high levels of satisfaction with the Alfalfa App, while also providing further suggestions for improvement.
Conclusions: The integration of "Internet+Pharmacy Care" using the Alfalfa App can improve the effectiveness of warfarin anticoagulation management in patients following heart valve surgery. The Alfalfa app provides a more efficient, secure, and cost-effective solution to warfarin management than traditional offline methods.
Keywords: alfalfa app; anticoagulation; internet + pharmacy care; mobile phone; smartphone; warfarin.
© Yiyi Qian, Weizhao Chen, Bin Zhou, Jiangya Li, Yuanyuan Guo, Zhiying Weng, Jinhua Zhang. Originally published in JMIR mHealth and uHealth (https://mhealth.jmir.org).
Conflict of interest statement
Figures
Similar articles
-
Effectiveness of the Alfalfa App in Warfarin Therapy Management for Patients Undergoing Venous Thrombosis Prevention and Treatment: Cohort Study.JMIR Mhealth Uhealth. 2021 Mar 2;9(3):e23332. doi: 10.2196/23332. JMIR Mhealth Uhealth. 2021. PMID: 33650976 Free PMC article.
-
Efficacy and safety of app-based remote warfarin management during COVID-19-related lockdown: a retrospective cohort study.J Thromb Thrombolysis. 2022 Jul;54(1):20-28. doi: 10.1007/s11239-021-02630-0. Epub 2022 Jan 29. J Thromb Thrombolysis. 2022. PMID: 35092566 Free PMC article.
-
New warfarin anticoagulation management model after heart valve surgery: rationale and design of a prospective, multicentre, randomised trial to compare an internet-based warfarin anticoagulation management model with the traditional warfarin management model.BMJ Open. 2019 Dec 5;9(12):e032949. doi: 10.1136/bmjopen-2019-032949. BMJ Open. 2019. PMID: 31811010 Free PMC article.
-
Sutureless Aortic Valve Replacement for Treatment of Severe Aortic Stenosis: A Single Technology Assessment of Perceval Sutureless Aortic Valve [Internet].Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2017 Aug 25. Report from the Norwegian Institute of Public Health No. 2017-01. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2017 Aug 25. Report from the Norwegian Institute of Public Health No. 2017-01. PMID: 29553663 Free Books & Documents. Review.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
References
-
- Chinese Society of Extracorporeal Circulation White book of Chinese cardiovascular surgery and extracorporeal circulation in 2019. Chinese Journal of Extracorporeal Circulation. 2020 Aug 28;20(4):196–199. doi: 10.13498/j.cnki.chin.j.ecc.2022.04.02. doi. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
