

Time to de-implementation of low-value cancer screening practices: a narrative review
- PMID: 40393787
- PMCID: PMC12322393
- DOI: 10.1136/bmjqs-2025-018558
Time to de-implementation of low-value cancer screening practices: a narrative review
Abstract
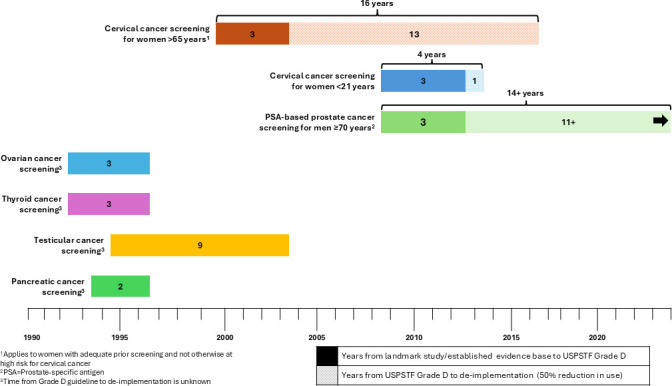
The continued use of low-value cancer screening practices not only represents healthcare waste but also a potential cascade of invasive diagnostic procedures and patient anxiety and distress. While prior research has shown it takes an average of 15 years to implement evidence-based practices in cancer control, little is known about how long it takes to de-implement low-value cancer screening practices. We reviewed evidence on six United States Preventive Services Task Force 'Grade D' cancer screening practices: (1) cervical cancer screening in women<21 years and >65 years, (2) prostate cancer screening in men≥70 years and (3) ovarian, (4) thyroid, (5) testicular and (6) pancreatic cancer screening in asymptomatic adults. We measured the time from a landmark publication supporting the guideline publication and subsequent de-implementation, defined as a 50% reduction in the use of the practice in routine care. The pace of de-implementation was assessed using nationally representative surveillance systems and peer-reviewed literature from the USA. We found the time to de-implementation of cervical cancer screening was 4 years for women<21 and 16 years for women>65. Prostate screening in men ≥70 has not reached a 50% reduction in use since the 2012 guideline release. We did not identify sufficient evidence to measure the time to de-implementation for ovarian, thyroid, testicular and pancreatic cancer screening in asymptomatic adults. Surveillance of low-value cancer screening is sparse, posing a clear barrier to tracking the de-implementation of these screening practices. Improving the systematic measurement of low-value cancer control practices is imperative for assessing the impact of de-implementation on patient outcomes, healthcare delivery and healthcare costs.
Keywords: Implementation science; Quality measurement; Standards of care.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
What is the value of routinely testing full blood count, electrolytes and urea, and pulmonary function tests before elective surgery in patients with no apparent clinical indication and in subgroups of patients with common comorbidities: a systematic review of the clinical and cost-effective literature.Health Technol Assess. 2012 Dec;16(50):i-xvi, 1-159. doi: 10.3310/hta16500. Health Technol Assess. 2012. PMID: 23302507 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Interventions targeted at women to encourage the uptake of cervical screening.Cochrane Database Syst Rev. 2021 Sep 6;9(9):CD002834. doi: 10.1002/14651858.CD002834.pub3. Cochrane Database Syst Rev. 2021. PMID: 34694000 Free PMC article.
-
Strategies for enhancing the implementation of school-based policies or practices targeting risk factors for chronic disease.Cochrane Database Syst Rev. 2017 Nov 29;11(11):CD011677. doi: 10.1002/14651858.CD011677.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2022 Aug 29;8:CD011677. doi: 10.1002/14651858.CD011677.pub3. PMID: 29185627 Free PMC article. Updated.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical