

Critical insights for intensivists on Guillain-Barré syndrome
- PMID: 40394364
- PMCID: PMC12092332
- DOI: 10.1186/s13613-025-01464-w
Critical insights for intensivists on Guillain-Barré syndrome
Abstract
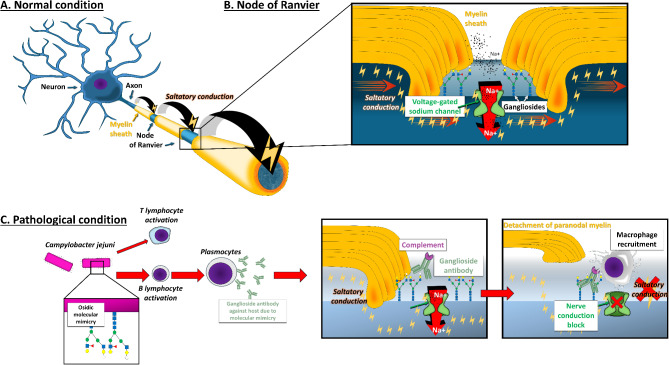
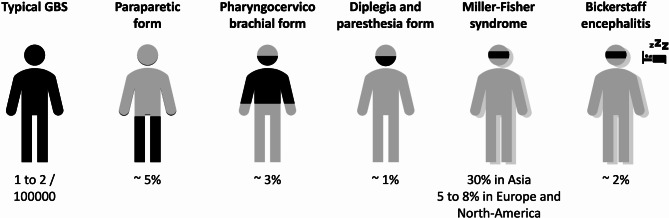
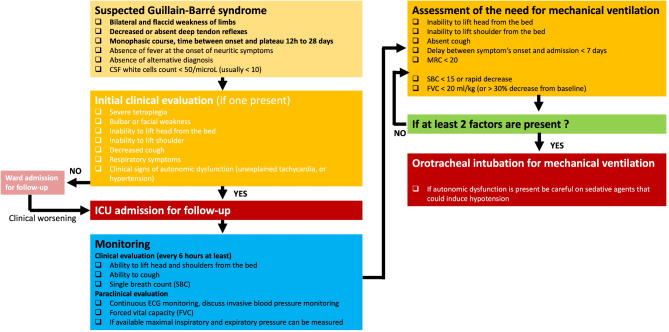
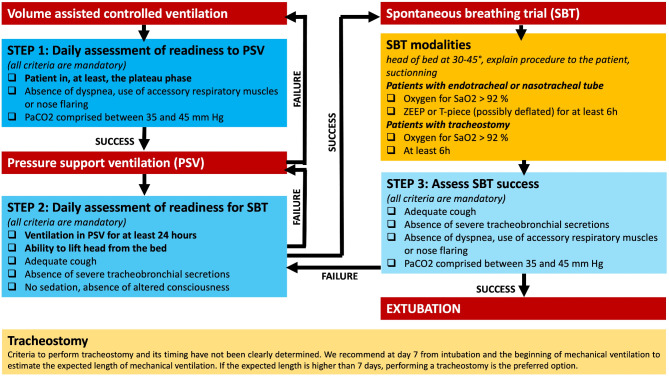
Guillain-Barré Syndrome (GBS) is a leading cause of acute flaccid tetraplegia worldwide, with an incidence of 1-2 cases per 100,000 people per year. Characterized by an immune-mediated polyneuropathy, GBS often follows infections or immunological triggers, including vaccinations. The syndrome is classified into three main subtypes based on electrophysiological findings: acute inflammatory demyelinating polyneuropathy (AIDP), acute motor axonal neuropathy (AMAN), and acute motor sensory axonal neuropathy (AMSAN). The pathophysiology of GBS involves molecular mimicry between microbial antigens and nerve structures, particularly affecting gangliosides and myelin proteins. Diagnosis primarily relies on clinical history, with lumbar puncture and electroneuromyogram used to confirm and differentiate subtypes. Treatment includes intravenous immunoglobulins or therapeutic plasma exchange associated with symptomatic treatment, especially mechanical ventilation if needed. Prognosis is generally favorable with a low mortality rate (< 5%) overall, but neurological sequelae can occur. Current research continues to explore novel therapeutic approaches, including complement-targeted therapies. Despite advancements, progress in specific treatments has been limited, and ongoing evaluation of potential biomarkers such as neurofilament light chains may enhance prognosis prediction and management strategies.
Keywords: Acute polyradiculoneuritis; Bickerstaff encephalitis; Guillain-Barré syndrome; Miller-Fisher.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable, review article. Consent for publication: Not applicable, review article. All authors consent to the submission of the current version of the manuscript. Competing interests: Nicolas Weiss perceived consultant fees from Owkin and Alexion. Clémence Marois perceived consultant fees from UCB.
Figures
References
-
- Yuki N, Hartung HP. Guillain-Barré syndrome. N Engl J Med. 2012;366(24):2294–304. - PubMed
-
- Willison HJ, Jacobs BC, van Doorn PA. Guillain-Barré syndrome. Lancet. 2016;388(10045):717–27. - PubMed
-
- Lu JL, Sheikh KA, Wu HS, Zhang J, Jiang ZF, Cornblath DR, et al. Physiologic-pathologic correlation in Guillain-Barré syndrome in children. Neurology. 2000;54(1):33–9. - PubMed
-
- Guillain G, Barré J, Strohl A. Sur Un syndromede radiculo-névrite avec hyperalbuminose du Liquide Céphalorachidien Sans réaction cellulaire. Remarques Sur les caractères cliniques et graphiques des réflexes tendineux. Bull et Mem de la Soc Méd des Hop de Paris. 1916;1462–70. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
