

Systemic outcomes of symptomatic peripheral artery disease patients with end-stage renal disease undergoing lower limb endovascular treatment: a propensity score-matched analysis
- PMID: 40394492
- PMCID: PMC12093713
- DOI: 10.1186/s12872-025-04838-x
Systemic outcomes of symptomatic peripheral artery disease patients with end-stage renal disease undergoing lower limb endovascular treatment: a propensity score-matched analysis
Abstract
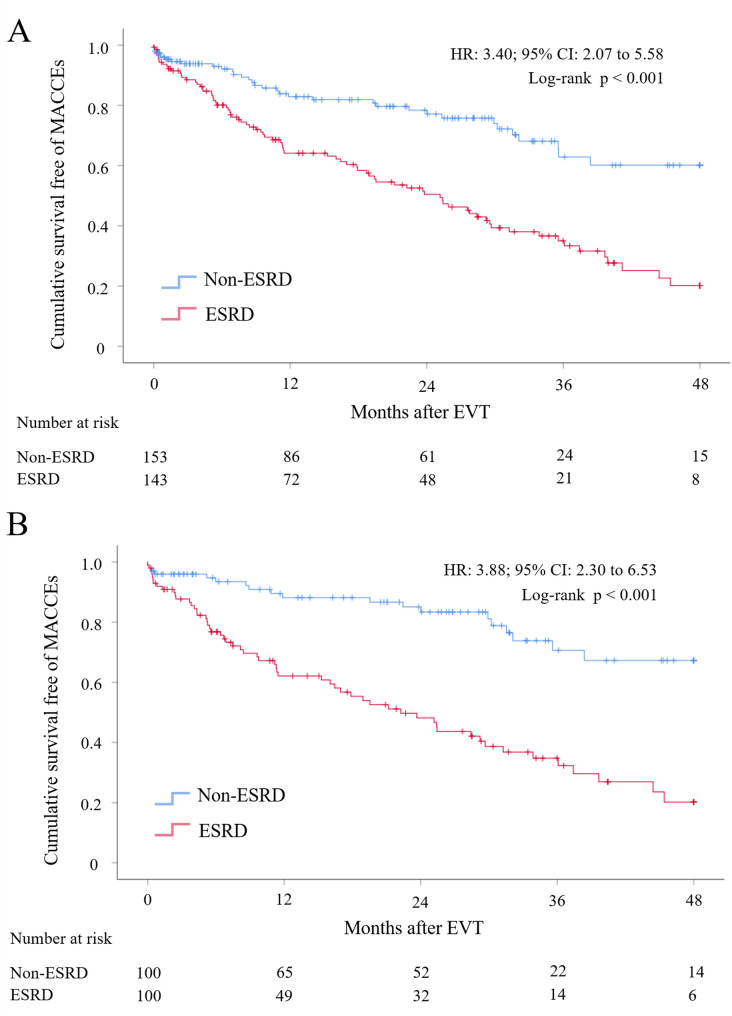
Background: This study investigates the impact of end-stage renal disease (ESRD) on systemic and localized outcomes in peripheral artery disease (PAD) patients following endovascular therapy (EVT), with a focus on major adverse cardiac and cerebrovascular events (MACCEs).
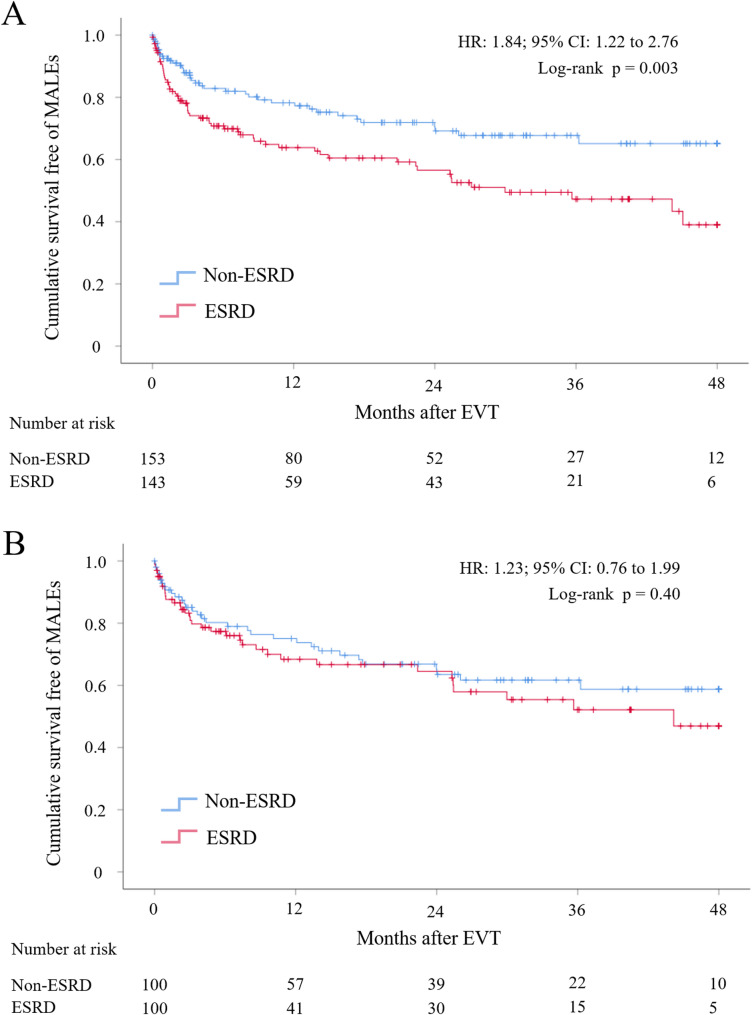
Methods: This retrospective cohort study included symptomatic PAD patients, categorized by the Rutherford classification, who underwent EVT at a single tertiary medical center from May 2018 to May 2021. Patients were divided into ESRD and non-ESRD groups. A propensity score-matched (PSM) analysis was performed to minimize confounding factors. The primary outcome was the occurrence of MACCEs, while the secondary outcome was the incidence of major adverse limb events (MALEs).
Results: ESRD patients exhibited significantly worse systemic outcomes, with higher MACCE rates compared to non-ESRD patients in both the entire cohort (79.9% vs. 39.9%; HR: 2.69; 95% CI: 1.80-4.02; p < 0.001) and the matched cohort (HR: 3.88; 95% CI: 2.30-6.53; p < 0.001). They also had higher rates of all-cause mortality and myocardial infarction (MI). For localized outcomes, MALEs were more frequent in the ESRD group in the entire cohort (61.0% vs. 34.9%; HR: 1.84; 95% CI: 1.22-2.76; p < 0.001), but no significant difference was observed in the matched cohort (HR: 1.23; 95% CI: 0.76-1.99; p = 0.40). ESRD was identified as the sole independent predictor of increased MACCE risk (HR: 2.49; 95% CI: 1.65-3.75; p < 0.001).
Conclusions: PAD patients with ESRD face significantly worse systemic outcomes, particularly elevated MACCE rates, after EVT. Preventing MACCEs, especially MI, is essential in this high-risk population. Despite more severe limb conditions, ESRD alone did not significantly increase MALE risk after PSM.
Clinical trial number: Not applicable.
Keywords: End-Stage renal disease; Endovascular interventions; MACCEs; MALEs; Peripheral artery disease; Systemic outcomes.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study adhered to the ethical guidelines of the 1975 Declaration of Helsinki. It was reviewed and approved by the Institutional Review Board of Chang Gung Medical Foundation (Institutional Review Board of Chang Gung Medical Foundation, IRB No: 202201849B0), which waived the need for an informed consent statement. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Clinical Outcomes Based on High Bleeding Risk in Patients With Lower Extremity Peripheral Artery Disease Who Have Undergone Endovascular Therapy.J Endovasc Ther. 2025 Apr;32(2):439-451. doi: 10.1177/15266028231176953. Epub 2023 May 29. J Endovasc Ther. 2025. PMID: 37246791
-
Chronic kidney disease and outcomes of lower extremity revascularization for peripheral artery disease.Atherosclerosis. 2020 Mar;297:149-156. doi: 10.1016/j.atherosclerosis.2019.12.016. Epub 2019 Dec 24. Atherosclerosis. 2020. PMID: 31948675 Free PMC article.
-
Open Versus Endovascular Revascularization of Below-Knee Arteries in Patients With End-Stage Renal Disease and Critical Limb Ischemia.Vasc Endovascular Surg. 2018 Nov;52(8):613-620. doi: 10.1177/1538574418789036. Epub 2018 Jul 18. Vasc Endovascular Surg. 2018. PMID: 30021493
-
Systematic review and meta-analysis of outcomes of lower extremity peripheral arterial interventions in patients with and without chronic kidney disease or end-stage renal disease.J Vasc Surg. 2021 Jan;73(1):331-340.e4. doi: 10.1016/j.jvs.2020.08.032. Epub 2020 Sep 1. J Vasc Surg. 2021. PMID: 32889074
-
The Double Burden: Deciphering Chronic Limb-Threatening Ischemia in End-Stage Renal Disease.Ann Vasc Surg. 2024 Oct;107:105-121. doi: 10.1016/j.avsg.2023.12.102. Epub 2024 Apr 9. Ann Vasc Surg. 2024. PMID: 38599491 Review.
References
-
- Kim HO, Kim J-M, Woo JS, Choi D, Ko Y-G, Ahn C-M, et al. Effects of chronic kidney disease on clinical outcomes in patients with peripheral artery disease undergoing endovascular treatment: analysis from the K-VIS ELLA registry. Int J Cardiol. 2018;262:32–7. - PubMed
-
- Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the united States: results from the National health and nutrition examination survey, 1999–2000. Circulation. 2004;110:738–43. - PubMed
-
- Rajagopalan S, Dellegrottaglie S, Furniss AL, Gillespie BW, Satayathum S, Lameire N, et al. Peripheral arterial disease in patients with end-stage renal disease. Circulation. 2006;114:1914–22. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
