

Inequities by race and ethnicity in cancer treatment receipt among people living with HIV and cancer in the U.S. (2004-2020)
- PMID: 40394520
- PMCID: PMC12090492
- DOI: 10.1186/s12885-025-14272-z
Inequities by race and ethnicity in cancer treatment receipt among people living with HIV and cancer in the U.S. (2004-2020)
Abstract
Objective: People with HIV (PWH) are less likely to receive cancer treatment compared to those without HIV. Social factors, such as cancer treatment facility type, which may impact cancer treatment receipt among PWH have not been quantitatively explored. Our objective was to characterize racial differences in social determinants of health (SDoH) that impact cancer treatment receipt among PWH and cancer in the US.
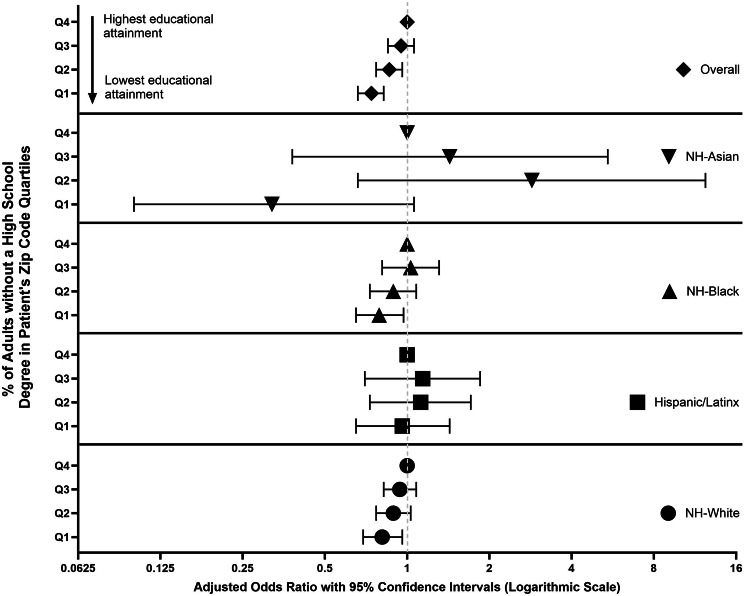
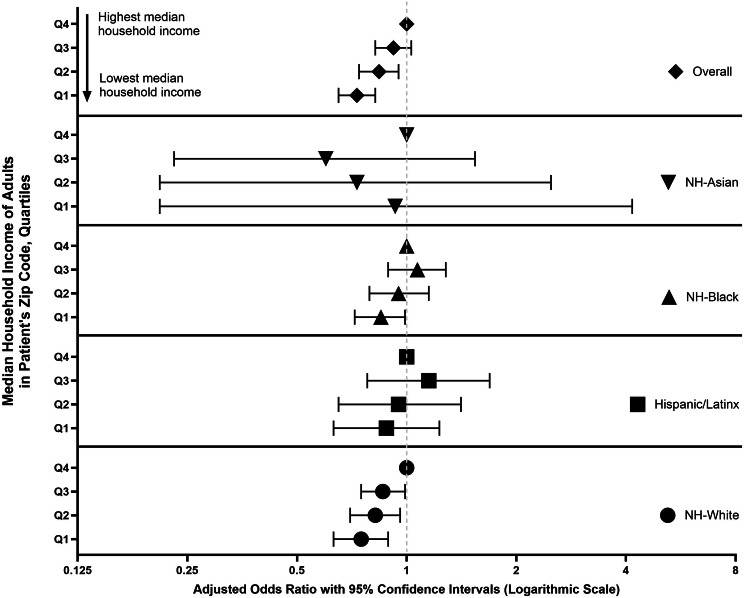
Methods: We used the National Cancer Database (2004-2020) and included adult (18-89 years) patients living with HIV identified using ICD9 and ICD10 codes. We included the 14 most common cancers that occur among PWH. Our main outcome was receipt of first-line cancer treatment, including systemic therapy, surgery, hormone therapy, and radiotherapy. Our main SDoH exposures included (1) area-level education or % of adults without a high school degree and (2) area-level income or median income quartiles within the patient's zip code. Healthcare access measures we evaluated included insurance status, distance to care, and cancer care facility type. We used hierarchical multivariable logistic regression models to estimate adjusted logistic ratios (aOR) with 95% confidence intervals (95% CI).
Results: We included 31,549 patients with HIV and cancer, of which 16% did not receive treatment. Overall, 43% of patients were aged ≥ 60 years, 38% were NH-Black, 68% were male, and 39% of patients resided in the South. 47% of patients were diagnosed with stage I/II cancer, and the most common cancers included were lung (21%), diffuse large B-cell lymphoma (12%), colorectal (9%) cancers, and prostate(9%). Compared to those in the highest quartile (Q4), PWH in the lower quartiles of educational attainment were less likely to receive cancer treatment (Q1 vs. Q4: aOR:0.74; 95% CI:0.66-0.82). Residing in the lower quartiles of household income was also inversely associated with cancer treatment receipt (Q1 vs.Q4: aOR:0.73; 95% CI:0.65-0.82). These associations were consistent among NH-White and NH-Black PWH. PWH living within 2 miles of their cancer care facility (vs. >45 miles away) and those treated at community cancer programs (vs. an academic/research program) were less likely to receive cancer treatment.
Conclusion: Area-level markers of social disadvantage are associated with cancer treatment receipt among PWH, suggesting SDoH factors may impact inequities in cancer treatment by HIV status.
Keywords: Cancer treatment; HIV; Immunotherapy; Inequities; Infectious diseases; Quality of care; Systemic therapy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The present analysis leverages existing secondary data collected by the American College of Surgeons. The data request supporting the present analysis was reviewed by Moffitt Cancer Center’s Scientific Review Committee (SRC) and deemed non-human subjects research. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
