

The feasibility and potential benefits of administering adjuvant chemotherapy in resected pancreatic cancer patients unable to promptly remove intraperitoneal drainage post-surgery: a retrospective cohort study
- PMID: 40394527
- PMCID: PMC12093592
- DOI: 10.1186/s12885-025-14262-1
The feasibility and potential benefits of administering adjuvant chemotherapy in resected pancreatic cancer patients unable to promptly remove intraperitoneal drainage post-surgery: a retrospective cohort study
Abstract
Objective: Pancreatectomy remains associated with a high incidence of complications. In certain cases, patients with pancreatic ductal adenocarcinoma (PDAC) face challenges in removing intraperitoneal drainage after surgery, leading to potential delays in the administration of adjuvant chemotherapy (AC) and potentially impacting survival outcomes. The objective of this study was to evaluate the feasibility and potential benefits of AC in PDAC patients who are unable to remove intraperitoneal drainage over 30 days.
Methods: Between January 2021 and December 2022, a total of 220 patients with resected PDAC received AC at our center. Among them, 84 patients experienced persistent intraperitoneal drainage lasting more than 30 days postoperatively. Of these, 38 patients (45.2%) initiated AC despite the ongoing presence of drainage and were classified as the AC(d+) group, while the remaining 46 patients (54.8%) began AC only after successful drainage removal, and were categorized as the AC(d-) group. The other 136 patients, who underwent prompt removal of intraperitoneal drainage, were assigned to the AC(pr) group. Baseline information, surgery-related outcomes, and chemotherapy-related adverse events were collected and compared between the two groups, and factors that affected recurrence-free survival (RFS) were also analysed.
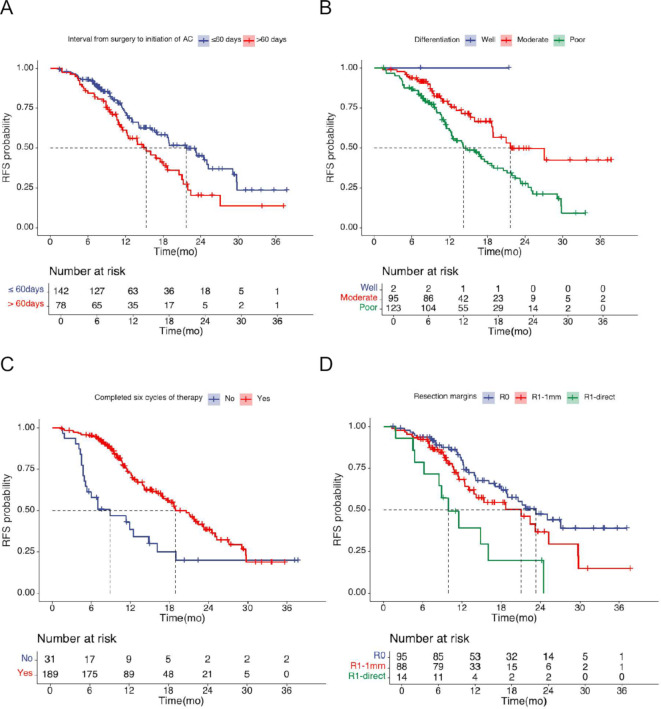
Results: Of the 220 patients included in the study, 107 (48.7%) experienced grade 3-4 chemotherapy-related adverse events. The interval from surgery to the initiation of AC was similar between the AC(d+) and AC(pr) groups (50 vs. 57 days, P = 0.108). However, it was significantly shorter in the AC(d+) group compared to the AC(d-) group (50 vs. 61 days, P = 0.015). Notably, no additional chemotherapy-related adverse events were observed in the AC(d+) group compared to either the AC(d-) or AC(pr) groups. The estimated 1-year and 2-year survival rates were 85.6% and 60.5%, respectively, for the AC(d-) group, and 95.8% and 61.0% for the AC(d+) group. In the AC(pr) group, the corresponding survival rates were 89.1% and 64.0%. Cox multivariate regression analysis demonstrated that tumour grade differentiation, completed six cycles of therapy, the interval from surgery to the initiation of AC and resection margins were independent factors affecting RFS.
Conclusion: Administering AC was safe for patients who underwent resection for PDAC and encountered challenges in the prompt removal of intraperitoneal drainage beyond 30 days post-surgery. The proactive management of preventing delays in chemotherapy administration could reduce the early recurrence risk in this particular patient cohort.
Keywords: Adjuvant chemotherapy; Intraperitoneal drainage; Pancreatic cancer; Postoperative pancreatic fistula; Recurrence-free survival.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: Ethics approval This study was approved by the Ethics Committee of the First Affiliated Hospital with Nanjing Medical University. Consent to participate: All patients signed an informed consent form. Competing interests: The authors declare no competing interests.
Figures
References
-
- Siegel RL, et al. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. - PubMed
-
- Marchegiani G, Bassi C. Prevention, prediction, and mitigation of postoperative pancreatic fistula. Br J Surg. 2021;108(6):602–4. - PubMed
-
- Valle JW, et al. Optimal duration and timing of adjuvant chemotherapy after definitive surgery for ductal adenocarcinoma of the pancreas: ongoing lessons from the ESPAC-3 study. J Clin Oncol. 2014;32(6):504–12. - PubMed
-
- Javed AA et al. A Delay in Adjuvant Therapy is Associated with Worse Prognosis only in Patients with Transitional Circulating Tumor Cells Following Resection of Pancreatic Ductal Adenocarcinoma. Ann Surg, 2022. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
