

Associations between pathological features and radioactive iodine-refractory recurrent papillary thyroid carcinoma: with mutation analysis using recurrent samples
- PMID: 40394531
- PMCID: PMC12090457
- DOI: 10.1186/s12902-025-01954-9
Associations between pathological features and radioactive iodine-refractory recurrent papillary thyroid carcinoma: with mutation analysis using recurrent samples
Abstract
Background: Although papillary thyroid carcinomas (PTC) are usually indolent in nature and clinically controllable, two-thirds of metastatic diseases become radioactive iodine-refractory (RAI-R). This study aimed to determine the role of pathological features, BRAFV600E, TERT promoter (TERT-p), and their combinations on Vietnamese patients with RAI-R recurrent PTC.
Methods: This cross-sectional study included 174 cases of locoregional recurrent PTC, including 135 and 39 RAI-R and RAI-avid (RAI-A) cases, respectively. Logistic regression analyses were used to evaluate the associations between pathological features, mutations, and RAI-R with tissues from recurrent lesions.
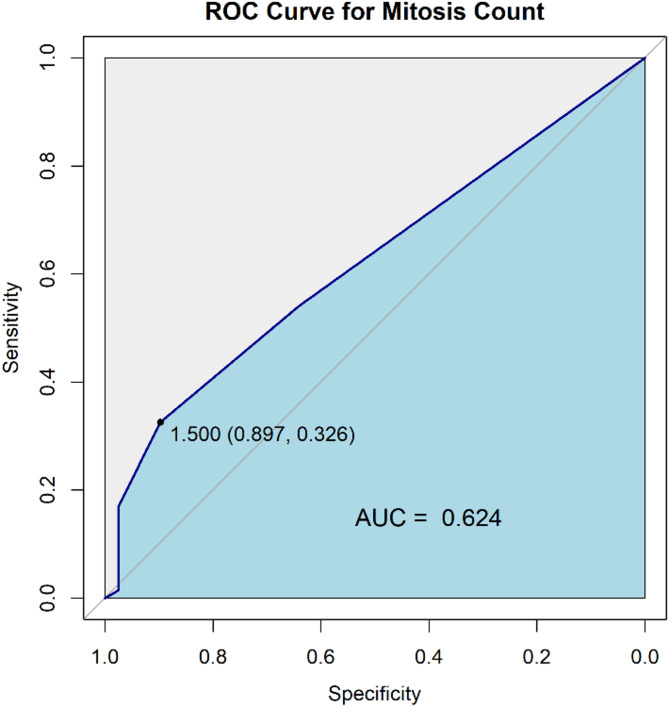
Results: Loss of polarity/loss of cell cohesiveness (LOP/LCC) component was exclusively observed in recurrent cancers in the RAI-R group. RAI-R was associated with BRAFV600E mutation, TERT-p mutation, BRAFV600E/TERT-p single mutant (Smut), BRAFV600E/TERT-p double mutant (Dmut), tall cell component, and mitosis ≥ 2/2 mm2 in the unadjusted logistic regression analysis. Multivariable logistic regression analysis revealed that BRAFV600E mutation and Dmut were independent predictors of RAI-R. The presence of Dmut (odds ratio [OR] = 6.64) was more significantly associated with RAI-R compared with that of Smut (OR = 2.75). There was a marginal association between tall cell > 5%, mitosis count ≥ 2/2 mm2 and RAI-R. The combination of BRAFV600E/tall cell components was the strongest predictor of RAI-R.
Conclusions: RAI-R PTC cases were independently associated with BRAFV600E, Dmut. The association between Dmut and RAI-R PTC was stronger than that between Smut and RAI-R PTC. Future studies should focus on elucidating the role of mitotic count and LOP/LCC in RAI-R PTC.
Keywords: BRAF V600E; TERT promoter; Mitosis; Radioactive iodine refractory; Recurrent papillary thyroid carcinoma; Tall cell.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of the 108 Military Central Hospital (5199/GCN-BV) and the Institutional Ethical Committee for Medical Research at Nagasaki University (#15062617-6). Informed consent was obtained from all participants. Consent to publish: Not applicable. Competing interests: The authors declare no competing interests. Clinical trial number: Not applicable.
Figures

Similar articles
-
The Genetic Duet of BRAF V600E and TERT Promoter Mutations Robustly Predicts Loss of Radioiodine Avidity in Recurrent Papillary Thyroid Cancer.J Nucl Med. 2020 Feb;61(2):177-182. doi: 10.2967/jnumed.119.227652. Epub 2019 Aug 2. J Nucl Med. 2020. PMID: 31375570 Free PMC article.
-
The genetic duet of BRAF V600E and TERT promoter mutations predicts the poor curative effect of radioiodine therapy in papillary thyroid cancer.Eur J Nucl Med Mol Imaging. 2022 Aug;49(10):3470-3481. doi: 10.1007/s00259-022-05820-x. Epub 2022 May 2. Eur J Nucl Med Mol Imaging. 2022. PMID: 35501518
-
Association Between Gross Features and Coexistence of BRAFV600E and TERT Promoter Mutations in Papillary Thyroid Carcinomas: A Combined Analysis Incorporating Clinicopathologic Features.Thyroid. 2024 Dec;34(12):1476-1485. doi: 10.1089/thy.2024.0310. Epub 2024 Oct 31. Thyroid. 2024. PMID: 39479802
-
BRAFV600E and TERT promoter C228T mutations on ThyroSeq v3 analysis of delayed skin metastasis from papillary thyroid cancer: a case report and literature review.World J Surg Oncol. 2023 Feb 17;21(1):49. doi: 10.1186/s12957-023-02937-7. World J Surg Oncol. 2023. PMID: 36804879 Free PMC article. Review.
-
Papillary thyroid carcinoma tall cell variant.Thyroid. 2008 Nov;18(11):1179-81. doi: 10.1089/thy.2008.0164. Thyroid. 2008. PMID: 18925842 Review.
Cited by
-
Gene Expression Analysis of Papillary Thyroid Carcinoma With Lymph Node Metastasis and Radioiodine Refractivity.Cureus. 2025 Jun 29;17(6):e87001. doi: 10.7759/cureus.87001. eCollection 2025 Jun. Cureus. 2025. PMID: 40746809 Free PMC article.
References
-
- Megwalu UC, Moon PK. Thyroid cancer incidence and mortality trends in the united States: 2000–2018. Thyroid. 2022;32:560–70. 10.1089/thy.2021.0662. - PubMed
-
- Schlumberger MJ. Papillary and follicular thyroid carcinoma. N Engl J Med. 1998;338:297–306. 10.1056/NEJM199801293380506. - PubMed
-
- Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, Caillou B, Ricard M, Lumbroso JD, De Vathaire F, et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab. 2006;91:2892–9. 10.1210/jc.2005-2838. - PubMed
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26:1–133. 10.1089/thy.2015.0020. - PMC - PubMed
-
- Filetti S, Durante C, Hartl DM, Leboulleux S, Locati LD, Newbold K, Papotti MG, Berruti A. clinicalguidelines@esmo.org EGCEa. ESMO clinical practice guideline update on the use of systemic therapy in advanced thyroid cancer. Ann Oncol. 2022;33:674–84. 10.1016/j.annonc.2022.04.009. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
