

Protective Effects of Bronchopulmonary Sequestration (BPS) on the Prognosis of Neonates with Congenital Diaphragmatic Hernia (CDH)
- PMID: 40394547
- PMCID: PMC12093729
- DOI: 10.1186/s12887-025-05755-w
Protective Effects of Bronchopulmonary Sequestration (BPS) on the Prognosis of Neonates with Congenital Diaphragmatic Hernia (CDH)
Abstract
Background: Congenital diaphragmatic hernia (CDH) and bronchopulmonary sequestration (BPS) are rare congenital anomalies that can coexist, with studies suggesting that 25-40% of CDH cases are accompanied by BPS. The association between CDH and BPS is thought to arise from embryological disruptions during early gestation, with BPS potentially serving as an anatomical barrier. This study aimed to evaluate the incidence, clinical characteristics, and outcomes of patients with concurrent CDH and BPS at a single institution to improve therapeutic approaches.
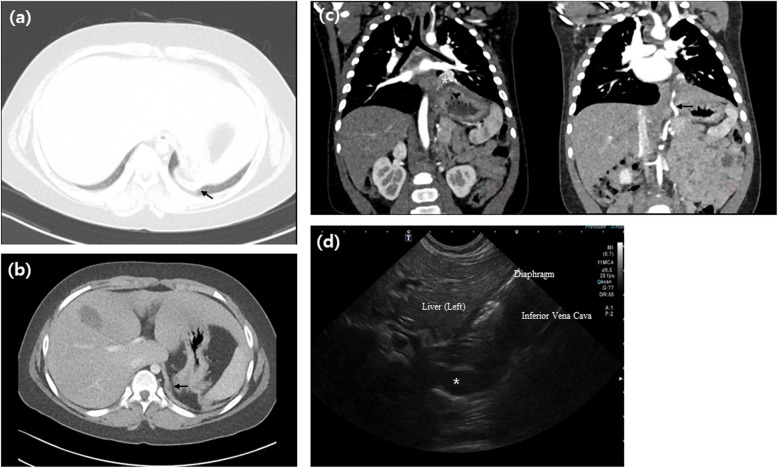
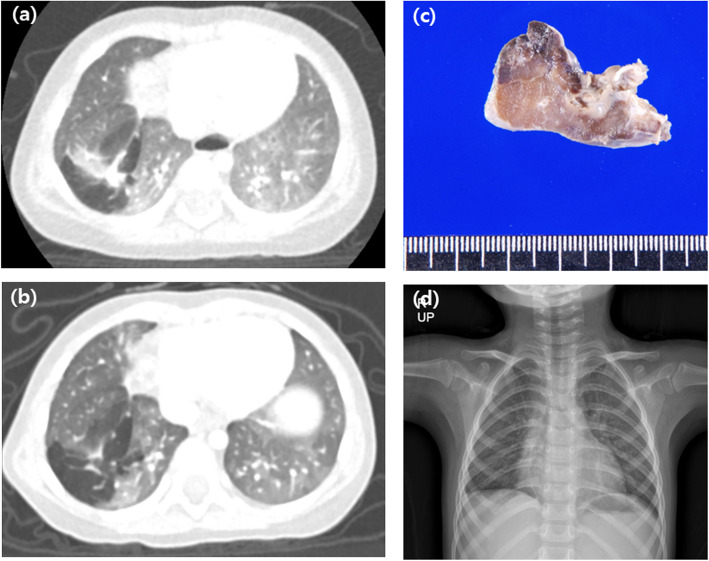
Methods: This study retrospectively analyzed the medical records of neonates diagnosed and treated for BPS concurrent with CDH at Asan Medical Center from 1990 to 2021, identifying 15 cases (3.0%) among 493 CDH patients. Comprehensive data on demographics, treatments, outcomes, diagnostic imaging, and pathological findings were collected and analyzed to explore disease characteristics and evaluate clinical outcomes.
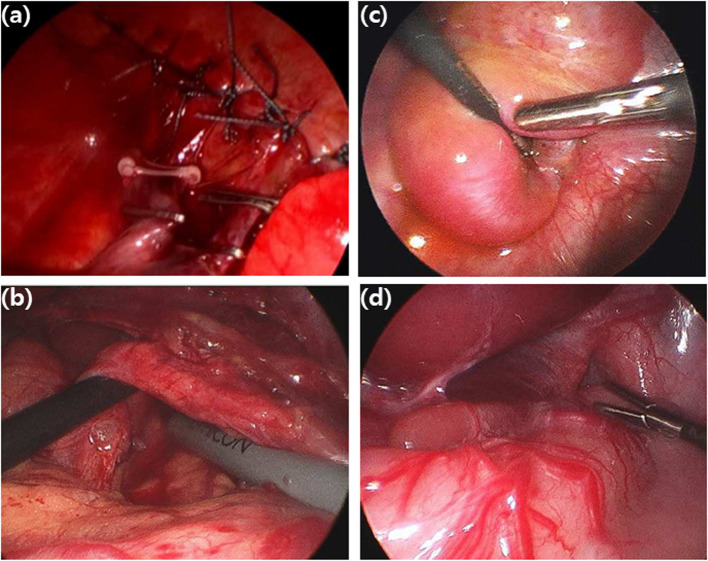
Results: This study analyzed 15 neonates with concurrent BPS and CDH, with a male predominance (10:5) and an average gestational age of 37.8 weeks, of whom 80% were diagnosed prenatally. CDH repair was performed at a median of 8 days, with no acute repair-related complications observed. In some cases, additional procedures such as hiatal hernia or re-do CDH repair was required, and BPS resection was performed either simultaneous or delayed. Follow-up revealed that most patients grew within the 50th percentile range, with thoracoscopic approaches feasible in over half of the cases, and recurrence-free outcomes achieved in those treated for hiatal hernia or BPS.
Discussions: No statistical difference in CDH severity was observed between the CDH and CDH + BPS groups, and the clinical outcome of CDH + BPS was better, although the high prevalence of sac-associated CDH types may have confounded the results. Our findings provide additional evidence supporting the protective effect of BPS. However, they also highlight the need for further studies in larger populations to clarify the causal relationship.
Keywords: Bronchopulmonary sequestration; Congenital diaphragmatic hernia; Diagnosis; Outcome; Surgery.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was approved by the Institutional Review Board of Asan Medical Center (IRB No.: 2022–0445). The requirement for informed consent was waived after the information was deidentified. This study was conducted in accordance with the principles of the Declaration of Helsinki. Consent for publication: Not applicable. As this is a retrospective study, informed consent for publication was waived. No identifiable images or clinical details that could potentially identify individual patients are included in this manuscript. Competing interests: The authors declare no competing interests.
Figures
References
-
- Alhamad M, Anand D. Congenital diaphragmatic hernia with associated broncho-pulmonary sequestration: A report of two cases and a literature review. J Neonatal Perinatal Med. 2024;17:123–31. 10.3233/NPM-230042. - PubMed
-
- Grethel EJ, Farrell J, Ball RH, Keller RL, Goldstein RB, Lee H, et al. Does congenital diaphragmatic hernia associated with bronchopulmonary sequestration portend a better prognosis? Fetal Diagn Ther. 2008;23:250–3. 10.1159/000123609. - PubMed
-
- Lee MY, Won HS, Shim JY, Lee PR, Lee BS, Kim EA, et al. Protective effect of fetal pulmonary sequestration in two cases of postnatal manifestation of congenital diaphragmatic hernia. Ultrasound Obstet Gynecol. 2012;39:719–22. 10.1002/uog.10099. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
