

Sex differences in out-of-hospital cardiac arrest
- PMID: 40395658
- PMCID: PMC12089750
- DOI: 10.1093/ehjopen/oeaf047
Sex differences in out-of-hospital cardiac arrest
Abstract
Aims: The impact of resuscitation care initiatives on sex-differences in out-of-hospital cardiac arrest (OHCA) survival remains unclear. We aim to examine sex-differences in characteristics and survival.
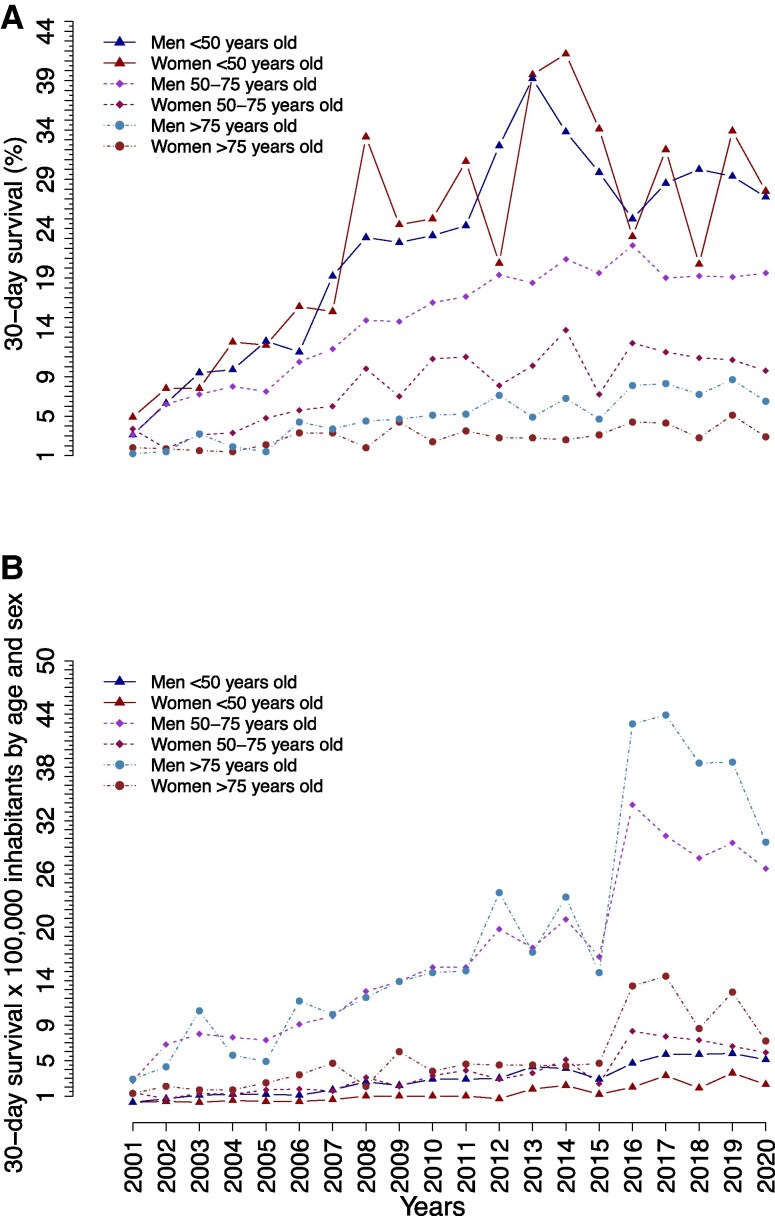
Methods and results: This Danish register-based study (2001-2020) included adult patients with a presumed cardiac cause of arrest. Temporal trends in survival were stratified by sex and subgroups: (i) bystander-witnessed status; (ii) bystander cardiopulmonary resuscitation (CPR); (iii) initial shockable heart rhythm; and age groups of <50, 50-75, and >75 years. To examine the association between sex and survival, we conducted adjusted logistic regression analyses. Among 50 066 OHCAs, women represented 34%. Women were older, had more chronic obstructive pulmonary disease, and lower prevalence of cardiovascular and cardiometabolic conditions than men. Women also had more OHCA at home (83.4 vs. 74.1%), fewer witnessed arrests (48.1 vs. 52.9%), half the probability of initial shockable heart rhythm (13.6 vs. 27.6%), and similar rates of receiving bystander-CPR. Survival rates improved over time for both sexes, but men had higher 30-day survival than women, even in subgroup and adjusted analyses [odds ratios (OR): 1.29; 95% confidence intervals (CI): 1.15-1.45, P < 0.001]. Sex-differences in survival were larger among those aged 50-75 years (in absolute and relative rates) and bystander witnessed arrests, while differences were smaller in those with initial shockable heart rhythms.
Conclusion: Despite increases in 30-day survival for both sexes, women consistently had lower survival rates than men. Sex-differences were larger among those aged 50-75 years or with bystander witnessed arrests, but smaller in the subset of patients with an initial shockable heart rhythm.
Keywords: 30-day survival; ESCAPE-NET; Female sex; Out-of-hospital cardiac arrest (OHCA); PARQ-COST; Women.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: Dr Zylyftari received grants from European Union’s Horizon 2020 research and innovation programme under acronym ESCAPE-NET, COST Action PARQ supported by COST (European Cooperation in Science and Technology), and Helsefonden. Dr Møller received grants from Karen Elise Jensen Fonden, Helsefonden and was employed by Novo Nordisk A/S after the project commenced. Novo Nordisk A/S is not engaged in this study. Dr Tan reports receiving grants from European Union’s Horizon 2020 research and innovation programme under acronym ESCAPE- NET (grant agreement no 733381), and COST Action PARQ supported by COST (European Cooperation in Science and Technology, grant agreement no CA19137). Dr Folke is supported by an unrestricted clinical research grant from the Novo Nordisk Foundation. Drs Gislason and Torp-Pedersen reports receiving grant support and honoraria from Bayer and Novo Nordisk. The remaining authors have no disclosures to report.
Figures




References
-
- Kragholm K, Wissenberg M, Mortensen RN., Hansen SM., Malta Hansen C, Thorsteinsson K, Rajan S, Lippert F, Folke F, Gislason G, Køber L, Fonager K, Jensen SE, Gerds TA, Torp-Pedersen C, Rasmussen BS. Bystander efforts and 1-year outcomes in out-of-hospital cardiac arrest. N Engl J Med 2017;376:1737–1747. - PubMed
-
- Bossaert L, Greif R, Maconochie I, Monsieurs KG, Nikolaou N, Nikolaou N, Nolan JP, Perkins GD, Soar J, Truhlář A, Wyllie J, Zideman D. Summary of the main changes in the Resuscitation Guidelines. ERC Guidelines 2015: European Resuscitation Council; 2015. https://cprguidelines.eu/assets/other-documents/ERC_summary_booklet_HRES... (9 May 2025).
-
- Rajan S, Wissenberg M, Folke F, Hansen SM, Gerds TA, Kragholm K, Hansen CM, Karlsson L, Lippert FK, Køber L, Gislason GH, Torp-Pedersen C. Association of bystander cardiopulmonary resuscitation and survival according to ambulance response times after out-of-hospital cardiac arrest. Circulation 2016;134:2095–2104. - PubMed
-
- Wissenberg M, Lippert FK, Folke F, Weeke P, Hansen CM, Christensen EF, Jans H, Hansen PA, Lang-Jensen T, Olesen JB, Lindhardsen J, Fosbol EL, Nielsen SL, Gislason GH, Kober L, Torp-Pedersen C. Association of National Initiatives to Improve Cardiac Arrest Management with rates of Bystander intervention and patient survival after out-of-hospital cardiac arrest. JAMA 2013;310:1377. - PubMed
LinkOut - more resources
Full Text Sources
