

A review of Mpox: Biological characteristics, epidemiology, clinical features, diagnosis, treatment, and prevention strategies
- PMID: 40395760
- PMCID: PMC12087419
- DOI: 10.1002/EXP.20230112
A review of Mpox: Biological characteristics, epidemiology, clinical features, diagnosis, treatment, and prevention strategies
Abstract
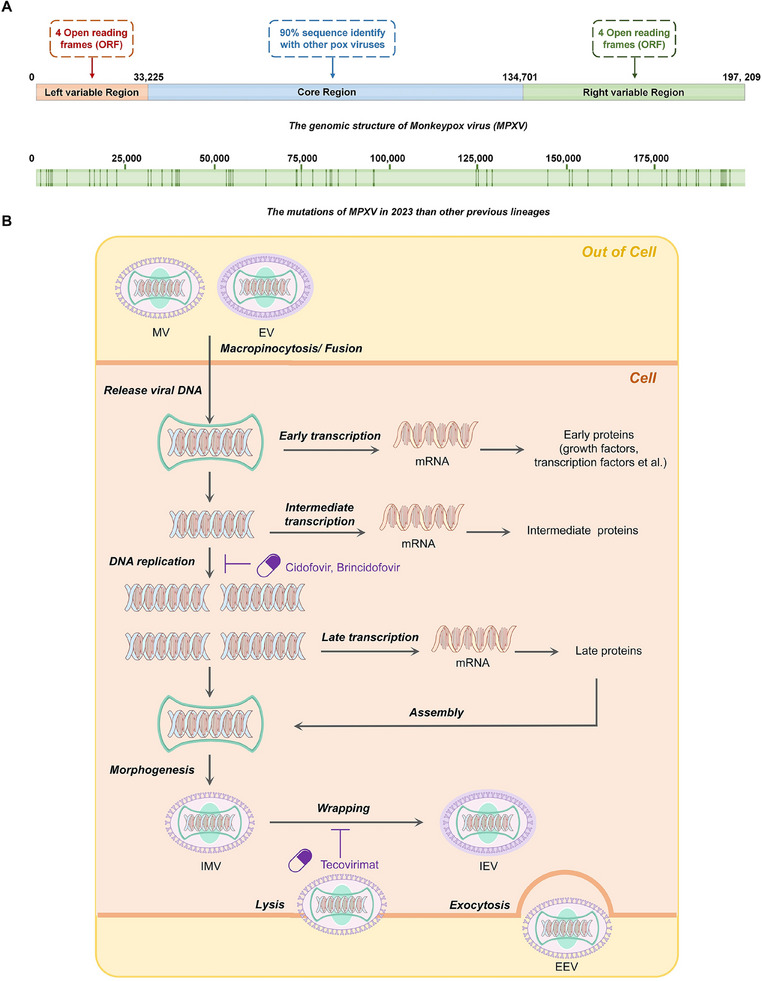
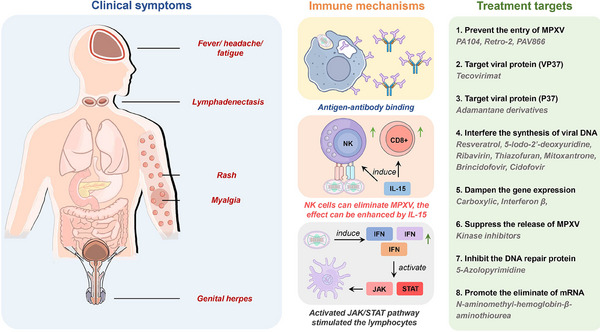
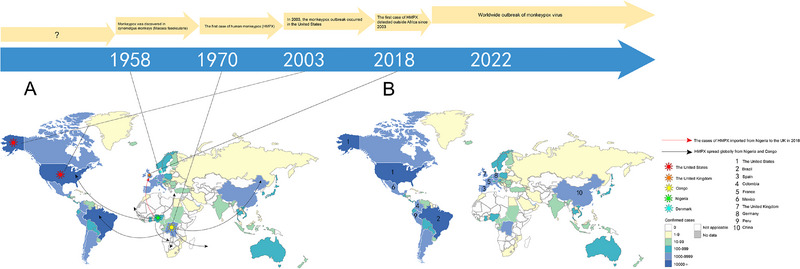
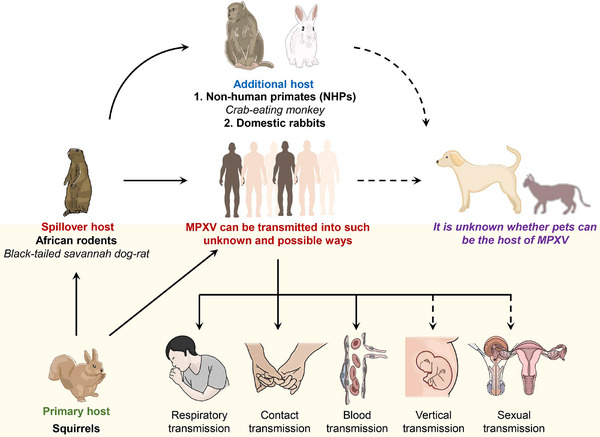
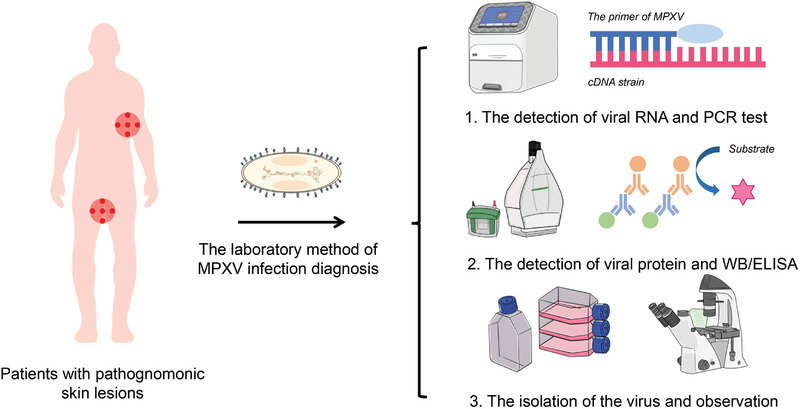
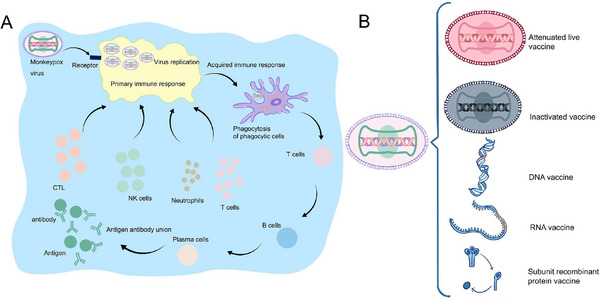
The outbreak of monkeypox virus (MPXV) was declared a Public Health Emergency of International Concern (PHEIC) by the World Health Organization (WHO), and the zoonotic disease caused by viral infection was renamed as "Mpox" on November 28, 2022. Currently, there is no approved vaccine or specific antiviral treatment for Mpox, and a main preventive strategy against MPXV infection remains the smallpox vaccine. Although there was an emergency use authorization (EUA) of Brincidofovir and Tecovirimat for the clinical treatment of clade II Mpox, while Tecovirimat failed to reduce the duration of Mpox lesions among patients infected with clade I Mpox in the Democratic Republic of the Congo (DRC). Therefore, it is still an urgent need to develop an effective medication. This review aims to enhance the understanding of Mpox and contribute to its prevention and treatment strategies, it provides a systemic introduction of the biological and epidemiological characteristics of MPXV, the clinical feature and diagnosis of Mpox, as well as treatment and prevention strategies, which will improve the comprehension about MPXV and offer potential strategies for clinical treatment.
Keywords: MPXV; Mpox; Orthopoxvirus; monkeypox; viral outbreak.
© 2024 The Author(s). Exploration published by Henan University and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Treatment efficacy of cidofovir and brincidofovir against clade II Monkeypox virus isolates.Antiviral Res. 2024 Nov;231:105995. doi: 10.1016/j.antiviral.2024.105995. Epub 2024 Sep 5. Antiviral Res. 2024. PMID: 39243894
-
Monkeypox Virus: WHO's Second Public Health Emergency of International Concern Within 2 Years.Microb Biotechnol. 2025 Apr;18(4):e70142. doi: 10.1111/1751-7915.70142. Microb Biotechnol. 2025. PMID: 40193168 Free PMC article. Review.
-
Mpox: emergence following smallpox eradication, ongoing outbreaks and strategies for prevention.Curr Opin Infect Dis. 2025 Jun 1;38(3):222-227. doi: 10.1097/QCO.0000000000001100. Epub 2025 Jan 29. Curr Opin Infect Dis. 2025. PMID: 39878084 Review.
-
Potential therapeutic targets for Mpox: the evidence to date.Expert Opin Ther Targets. 2023 Jan-Jun;27(6):419-431. doi: 10.1080/14728222.2023.2230361. Epub 2023 Jul 4. Expert Opin Ther Targets. 2023. PMID: 37368464 Free PMC article.
-
Mpox Virus and its ocular surface manifestations.Ocul Surf. 2024 Oct;34:108-121. doi: 10.1016/j.jtos.2024.07.001. Epub 2024 Jul 5. Ocul Surf. 2024. PMID: 38972544 Review.
References
Publication types
LinkOut - more resources
Full Text Sources