

Methylprednisolone for Infant Heart Surgery: Subpopulation Analyses of a Randomized Controlled Trial
- PMID: 40396812
- PMCID: PMC12378003
- DOI: 10.1097/CCM.0000000000006721
Methylprednisolone for Infant Heart Surgery: Subpopulation Analyses of a Randomized Controlled Trial
Abstract
Objectives: Evaluate benefits and harms of prophylactic intraoperative methylprednisolone in subpopulations undergoing infant heart surgery.
Design: Subpopulation analyses of The Steroids to Reduce Systemic Inflammation after Infant Heart Surgery (STRESS) trial, a double-blind randomized placebo-controlled trial.
Setting: Twenty-four congenital heart centers.
Patients: Infants (< 1 yr old) undergoing heart surgery with cardiopulmonary bypass. Patients stratified by Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery Congenital Heart Surgery (STAT) mortality category, age, gestational age, and presence of chromosomal or syndromic diagnosis (CSD).
Interventions: Methylprednisolone (30 mg/kg) vs. placebo administered into cardiopulmonary bypass pump-priming fluid.
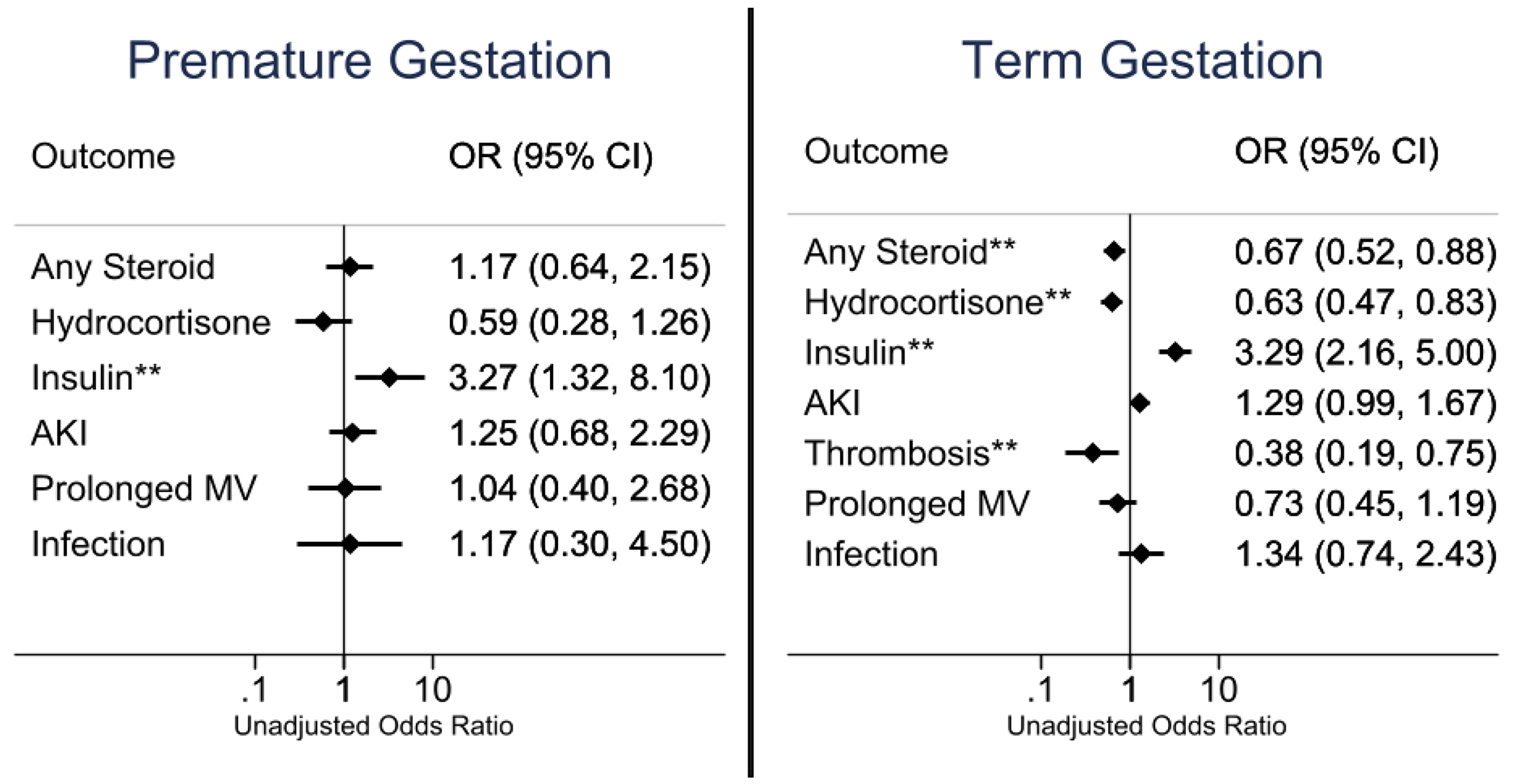
Measurements and main results: Six postoperative outcomes: steroid use, acute kidney injury (AKI), thrombosis, infections, prolonged mechanical ventilation, peak blood glucose levels, and insulin exposure. One thousand two hundred patients received methylprednisolone or placebo. Beneficial effects associated with methylprednisolone included reduced use of postoperative hydrocortisone in neonates (odds ratio [OR], 0.39 [0.25-0.60]), both STAT category groups (1-3: OR, 0.64 [0.46-0.89]; 4-5: OR, 0.57 [0.34-0.97]), term infants (OR, 0.63 [0.47-0.83]), and those without CSD (OR, 0.63 [0.46-0.86]). Methylprednisolone was associated with lower thrombosis occurrence among neonates (OR, 0.37 [0.16-0.87]) and term infants (OR, 0.38 [0.19-0.75]). Adverse associations included increased thrombosis among premature infants ( p = 0.005), increased AKI among neonates (OR, 1.55 [1.02-2.37]) and those following STAT category 1-3 operations (OR, 1.34 [1.02-1.75]), and increased peak blood glucose levels and insulin exposure (all subgroups; p < 0.001). No increase in overall infection or reduction in prolonged mechanical ventilation with methylprednisolone.
Conclusions: Both beneficial and adverse associations were observed with prophylactic methylprednisolone. Reduction in postoperative hydrocortisone administration and absence of increased infection rates are arguments favoring prophylactic methylprednisolone use. Methylprednisolone was associated with increased peak blood glucose levels and a neutral to harmful association with odds of AKI. These data suggest certain subpopulations may benefit from prophylactic intraoperative methylprednisolone without significant harm.
Keywords: cardiac surgery; congenital heart disease; critical care; methylprednisolone.
Copyright © 2025 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Drs. Sunthankar, Hill, J. P. Jacobs, Li, Graham, Benscoter, Van Bergen, Scott, Anderson, and Kannankeril received support for article research from the National Institutes of Health (NIH). Dr. Hill’s institution received funding from the National Center for Advancing Translational Sciences (NCATS); he received funding from Bristol Myers Squibb and Johnson & Johnson. Dr. M. L. Jacobs’ institution received funding from the NCATS (U01TR001803). Drs. Van Bergen’s, Anderson’s, and Kannakeril’s institutions received funding from the NIH. Dr. Anderson’s institution received funding from the National Heart, Lung, and Blood Institute (R01HL140055; UM1 4833193) and Autus. Dr. Anderson was a consultant for Autus Valve Technologies. Dr. J. P. Jacobs was a consultant for SpecialtyCare. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures



References
-
- Jacobs JP, Mayer JE Jr., Pasquali SK et al. The Society of Thoracic Surgeons Congenital Heart Surgery Database: 2019 Update on Outcomes and Quality. Ann Thorac Surg 2019;107:691–704. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
