

Epidemiology of Valvular Heart Disease in Asia Pacific Region
- PMID: 40396937
- PMCID: PMC12287747
- DOI: 10.1016/j.jacasi.2025.03.011
Epidemiology of Valvular Heart Disease in Asia Pacific Region
Abstract
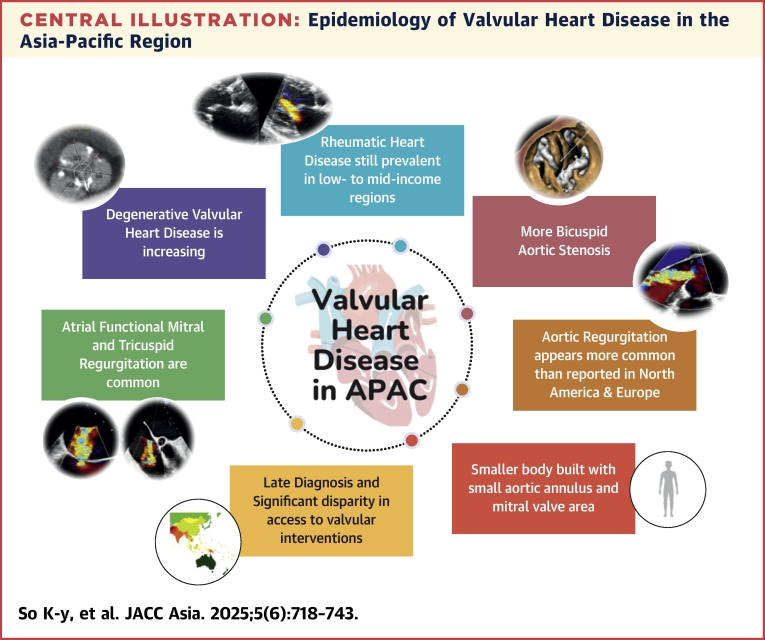
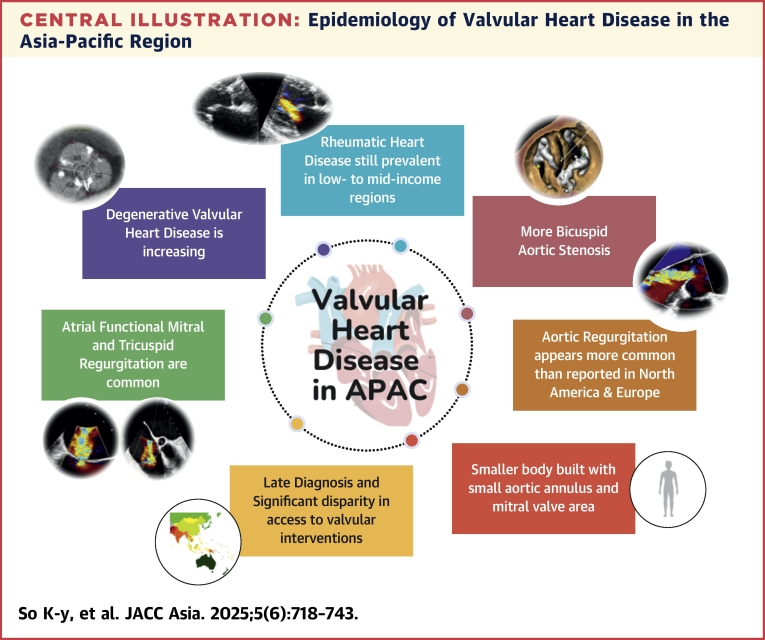
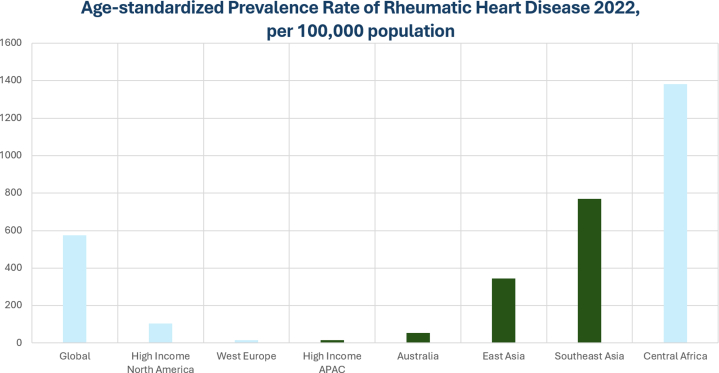
Valvular heart disease poses a significant health burden in the Asia-Pacific region, with its epidemiology varying widely across countries caused by diverse socioeconomic and health care situations. Rheumatic heart disease remains prevalent, especially in low- to middle-income areas, while degenerative valvular diseases are emerging in developed regions caused by an aging population. Significant disparities in access to health care and intervention result in variable clinical outcomes. In the past decade, transcatheter interventions have revolutionized the management of patients with valvular heart disease globally. In the Asia-Pacific region, the uptake and development of transcatheter valvular interventions has been slow until recent years. Continued collaboration across the Asia-Pacific region is essential to mitigate the impact of the upcoming surge of valvular heart disease in this diverse and rapidly changing area.
Keywords: Asia Pacific; degenerative valve disease; diagnosis; epidemiology; rheumatic heart disease; valvular heart disease.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The authors received no financial support for the research, authorship, and/or publication of this paper. Dr So is a clinical proctor for Abbott, Boston Scientific, Edwards Lifescience, and Medtronic. Dr Yap has received speaker honoraria from Biosensors, Biotronik, Boston Scientific, Edwards Lifesciences, Johnson and Johnson, Kaneka, Medtronic, and Terumo. Dr Poon is a consultant for Edwards Lifesciences; has received institutional research grants from Abbott, Medtronic, and Edwards Lifesciences; and has received travel support from Edwards Lifesciences and Medtronic. Dr Chandavimol is a clinical proctor for Edwards Lifesciences, Boston Scientific, Abbott, and Medtronic. Dr Hayashida is a clinical proctor for Edwards Lifesciences, Medtronic, and Abbott. Dr Ewe has received speaker fees from Abbott Medical, Philips, and GE HealthCare. Dr Chen has received grants from Boston Scientific and Edwards Lifesciences; and is a consultant for Jenscare Scientific. Dr Ohno is a clinical proctor for Abbott and Medtronic. Dr Hon is a clinical proctor for Edwards and Medtronic; and has received speaker honorarium from Edwards and Medtronic. DrBhagwandeen is a proctor for Edwards Lifesciences and Medtronic. Dr Tabata is a clinical proctor for Medtronic, Abbott, and Edwards Lifescience; and has received a research grant from Medtronic and Abbott. Prof Lee has received a research grant from Abbott and Philips. Dr Jilaihawi has received an institutional clinical research grant from Pi-Cardia; is a consultant to Edwards Lifesciences and Medtronic; and is an investor in DASI simulations. Dr Wang is a consultant for Abbott, Boston Scientific, Edwards Lifesciences, Materialise, and NeoChord. Dr Tang has received speaker's honoraria and served as a physician proctor, consultant, advisory board member, TAVR publications committee member, RESTORE study steering committee member, APOLLO trial screening committee member, and IMPACT MR steering committee member for Medtronic; has received speaker's honoraria and served as a physician proctor, consultant, advisory board member and TRILUMINATE trial anatomic eligibility and publications committee member for Abbott Structural Heart; has served as an advisory board member for Boston Scientific; has served as a consultant and physician screening committee member for Shockwave Medical; has served as a consultant for Philips and Edwards Lifesciences, Peijia Medical and Shenqi Medical Technology; and has received speaker's honoraria from Siemens Healthineers. Dr Lim has received consultant fees/honoraria from Ancora, Dinova Medtech, Valgen, Venus, W. L. Gore and Associates Inc; and is a coinvestigator in Abbott COAPT, REPAIR-MR and TRILUMINATE, Edwards CLASP IID/F, and Medtronic APOLLO clinical trials. Dr Modine has received administrative support, article publishing charges, statistical analysis, and writing assistance from Medtronic; has served as a consultant or advisor for Abbott, Medtronic, Microport, Edwards Lifesciences, and Jenscare Scientific Co; and has received funding grants from Medtronic and Edwards Lifesciences. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Izumi C., Matsuyama R., Asaoka M., et al. Valvular heart disease in Japan: Characteristics and treatment of patients in acute care hospitals in 2019. J Cardiol. 2023;82:29–34. - PubMed
-
- Watkins D.A., Johnson C.O., Colquhoun S.M., et al. Global, regional, and national burden of rheumatic heart disease, 1990–2015. N Engl J Med. 2017;377:713–722. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
