

Transcutaneous Cervical Vagus Nerve Stimulation Improves Speech Comprehension in Noise: A Crossover, Placebo-Controlled Study
- PMID: 40396942
- PMCID: PMC12269552
- DOI: 10.1016/j.neurom.2025.04.007
Transcutaneous Cervical Vagus Nerve Stimulation Improves Speech Comprehension in Noise: A Crossover, Placebo-Controlled Study
Abstract
Background: Speech comprehension in noisy environments remains a significant challenge, even among individuals with clinically normal hearing and users of hearing aids and cochlear implants. Although conventional assistive hearing devices address limitations in the auditory periphery, they do not directly enhance the brain's capacity to segregate speech from background noise. Because tonic vagus nerve stimulation (VNS) has shown potential for rapidly improving central sensory processing, this study investigated whether tonic transcutaneous cervical VNS (tcVNS) can enhance speech-in-noise intelligibility.
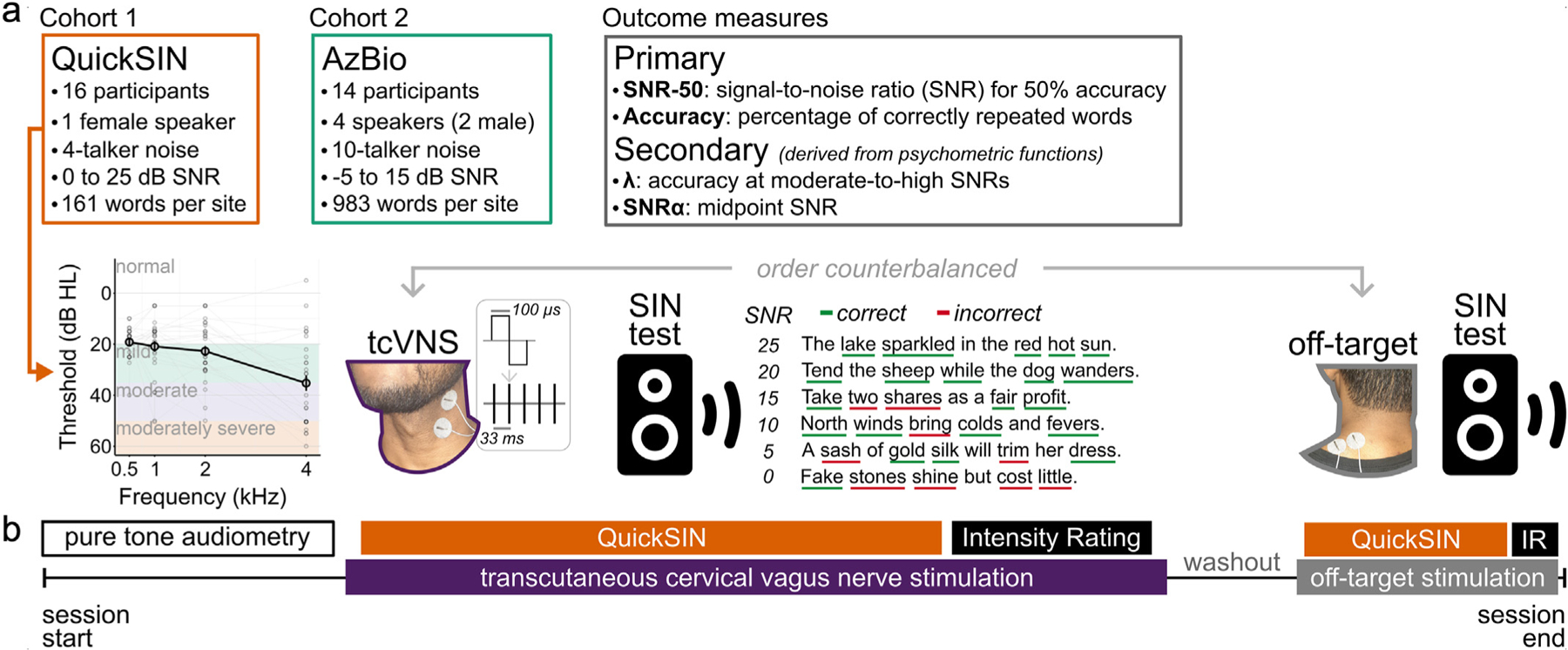
Materials and methods: Two cohorts of older human adults (aged 60-84 years) participated in a placebo-controlled, crossover study. Participants completed speech-in-noise assessments using either QuickSIN or AzBio sentences while receiving tonic tcVNS to the neck, or placebo stimulation to the neck-shoulder junction. Speech-in-noise performance was assessed by measuring participants' accuracy in repeating sentences presented at varying signal-to-noise ratios (SNR) within background babble.
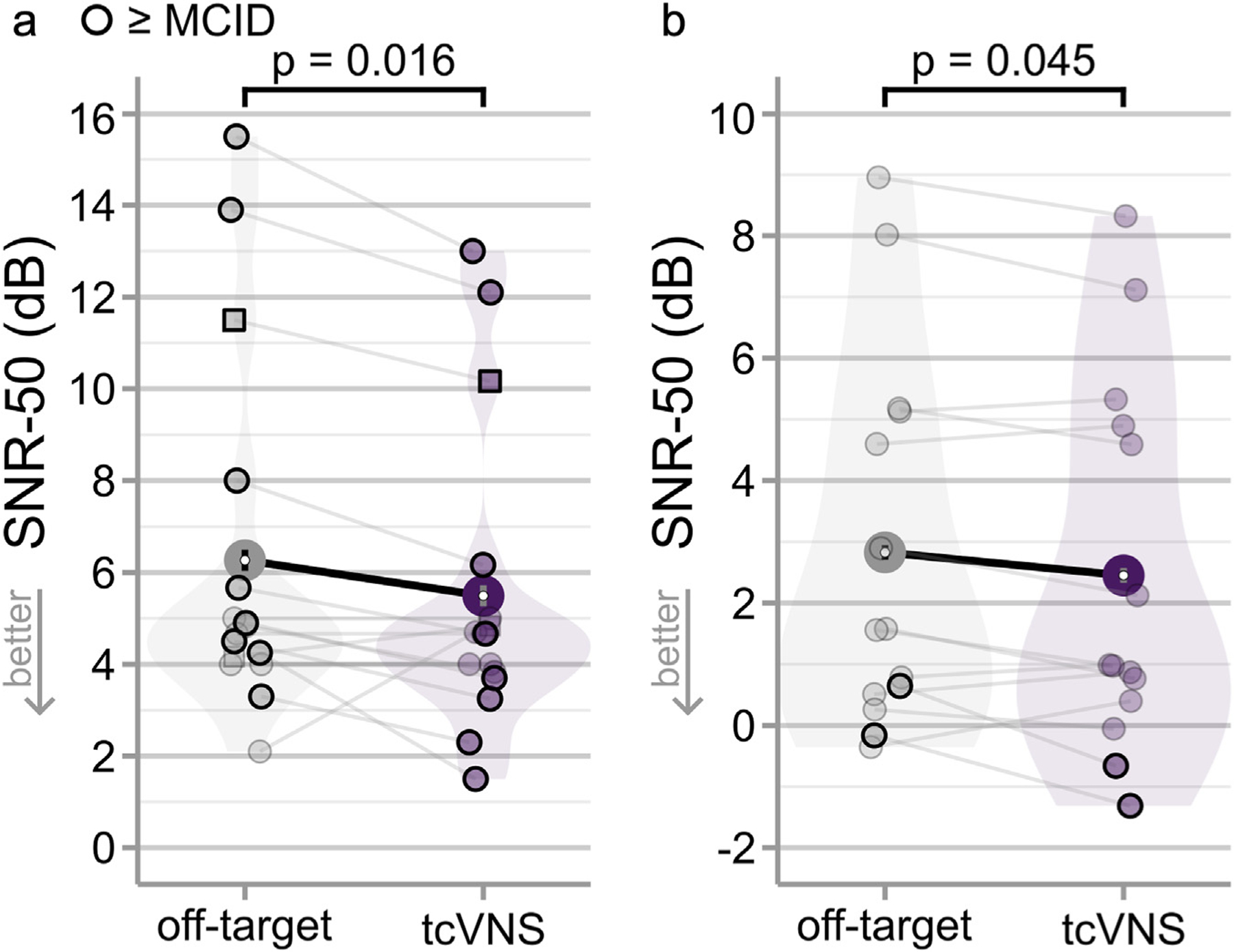
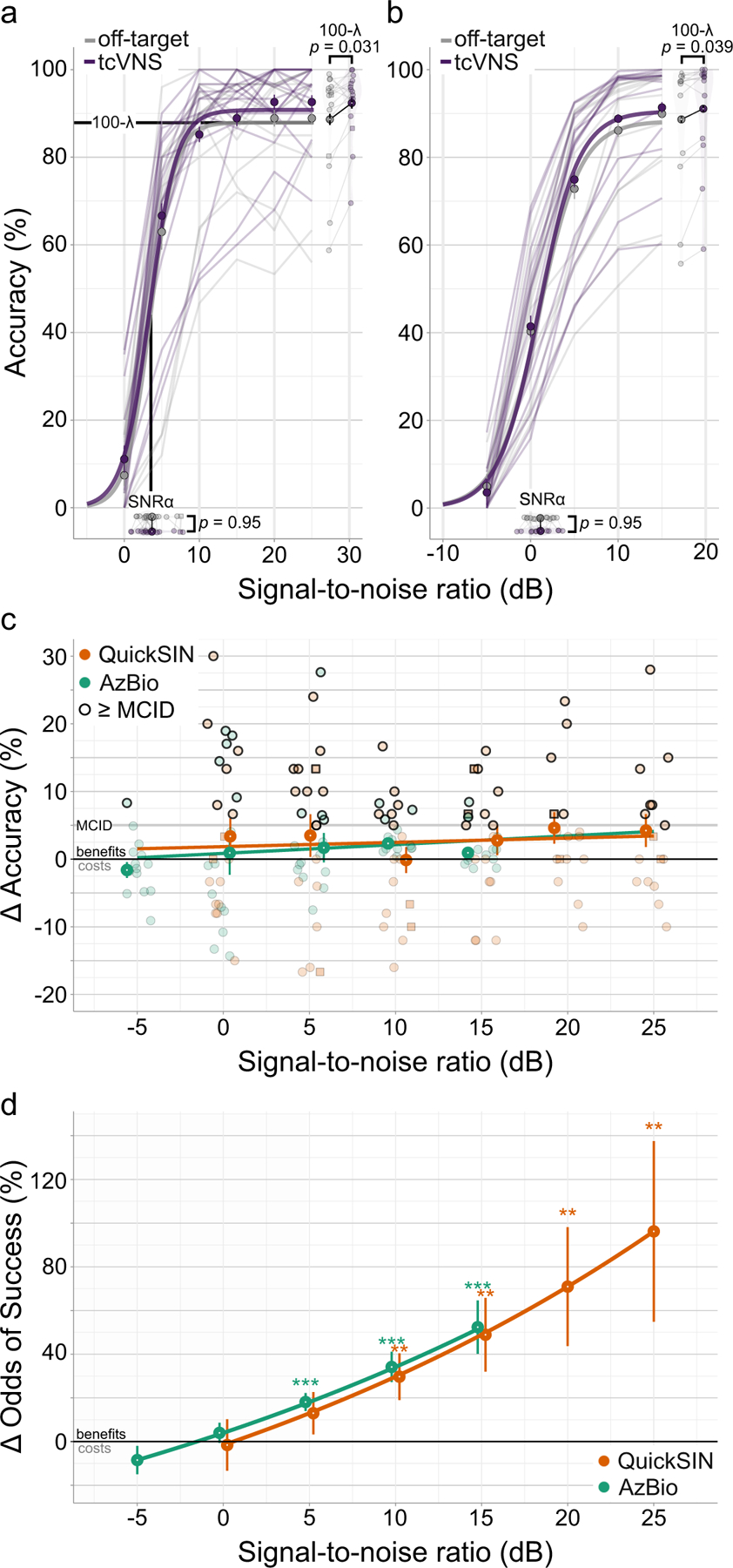
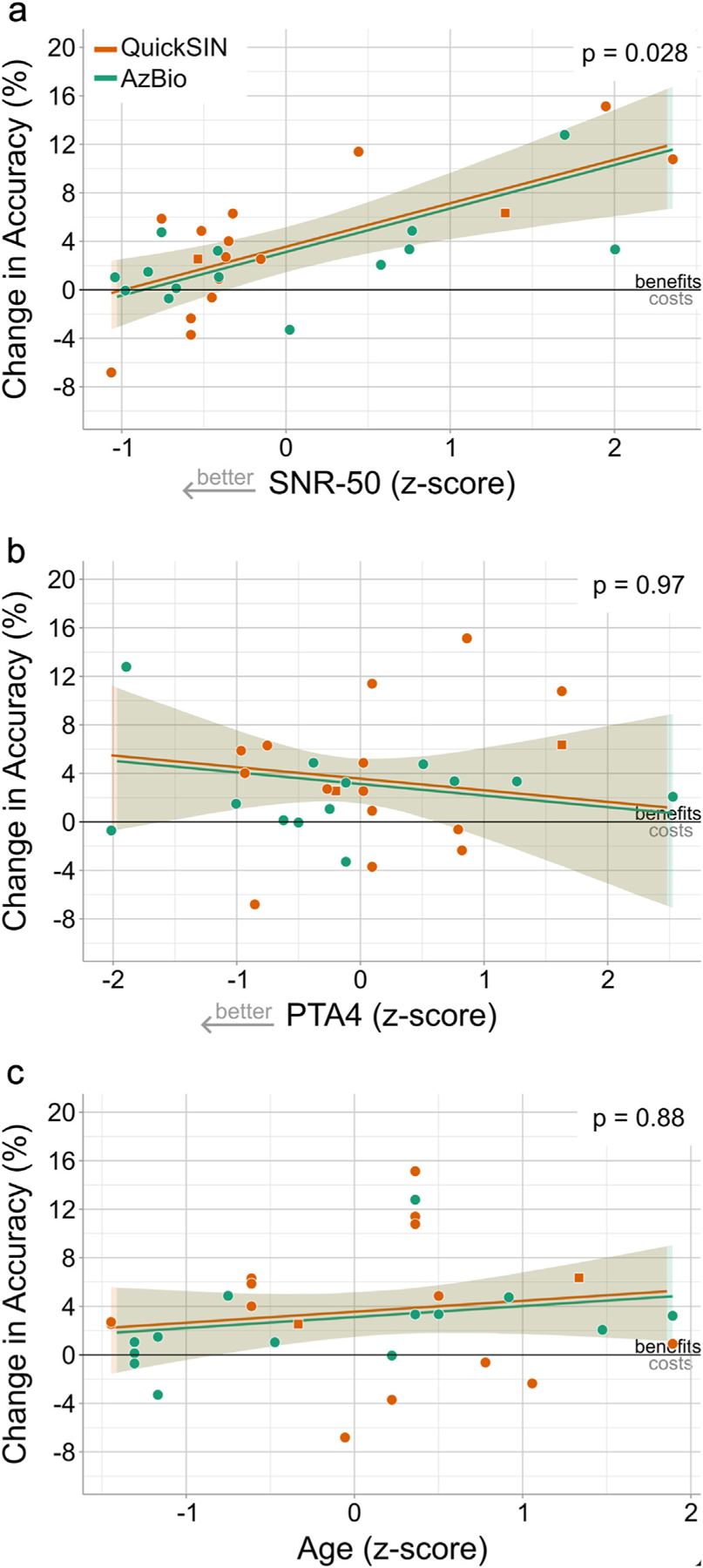
Results: Tonic tcVNS improved speech-in-noise intelligibility compared with placebo. At the group level, the SNR threshold for 50% speech intelligibility (SNR-50) improved by 0.76 dB in QuickSIN (p = 0.016) and by 0.38 dB in AzBio (p = 0.045). For individual participants, 50% showed improvements that met a minimum clinically important difference (MCID) of 1 dB. Tonic tcVNS evoked progressively greater improvements as SNR increased in QuickSIN (p = 0.021) and AzBio (p = 0.00023), with the largest gains at SNRs >0 dB. In 55% of participants, tcVNS improved intelligibility beyond an MCID benchmark of 4.9% at 5 dB SNR. Although the magnitude of tcVNS-evoked improvements was inversely related to baseline speech-in-noise impairment (p = 0.028), with the individuals having the most impaired speech-in-noise intelligibility showing the largest gains, it did not correlate with hearing loss severity (p = 0.97) or age (p = 0.88).
Conclusions: Our findings indicate that tonic tcVNS can evoke immediate and clinically meaningful enhancements in speech-in-noise comprehension. This suggests tcVNS may complement conventional assistive hearing technologies and inform novel therapies for sensory processing disorders.
Keywords: Aging; locus coeruleus; norepinephrine; speech in noise; vagus nerve stimulation.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest All authors are stockholders in Sharper Sense, Inc, a company developing methods for enhancing sensory processing with vagus nerve stimulation. Jason B. Carmel is a founder and stockholder in BackStop Neural and has received honoraria from Pacira, Motric Bio, and Restorative Therapeutics.
Figures
Update of
-
Transcutaneous cervical vagus nerve stimulation improves speech comprehension in noise: A crossover, placebo-controlled study.bioRxiv [Preprint]. 2025 Mar 25:2024.12.10.627804. doi: 10.1101/2024.12.10.627804. bioRxiv. 2025. Update in: Neuromodulation. 2025 May 21:S1094-7159(25)00151-5. doi: 10.1016/j.neurom.2025.04.007. PMID: 40196667 Free PMC article. Updated. Preprint.
Similar articles
-
Transcutaneous cervical vagus nerve stimulation improves speech comprehension in noise: A crossover, placebo-controlled study.bioRxiv [Preprint]. 2025 Mar 25:2024.12.10.627804. doi: 10.1101/2024.12.10.627804. bioRxiv. 2025. Update in: Neuromodulation. 2025 May 21:S1094-7159(25)00151-5. doi: 10.1016/j.neurom.2025.04.007. PMID: 40196667 Free PMC article. Updated. Preprint.
-
The relationships between cochlear nerve health and AzBio sentence scores in quiet and noise in postlingually deafened adult cochlear implant users.medRxiv [Preprint]. 2025 Apr 28:2024.11.16.24317332. doi: 10.1101/2024.11.16.24317332. medRxiv. 2025. PMID: 39606331 Free PMC article. Preprint.
-
Hearing Instruments for Unilateral Severe-to-Profound Sensorineural Hearing Loss in Adults: A Systematic Review and Meta-Analysis.Ear Hear. 2016 Sep-Oct;37(5):495-507. doi: 10.1097/AUD.0000000000000313. Ear Hear. 2016. PMID: 27232073 Free PMC article.
-
Degradation in Binaural and Spatial Hearing, and Auditory Temporal Processing Abilities, as a Function of Aging.bioRxiv [Preprint]. 2025 Feb 20:2024.07.08.602575. doi: 10.1101/2024.07.08.602575. bioRxiv. 2025. PMID: 39026701 Free PMC article. Preprint.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
References
-
- Van Hedger SC, Johnsrude IS. Speech perception under adverse listening conditions. In: Holt LL, Peelle JE, Coffin AB, Popper AN, Fay RR, eds. Speech Perception. Springer; 2022:141–171.
-
- Spankovich C, Gonzalez VB, Su D, Bishop CE. Self reported hearing difficulty, tinnitus, and normal audiometric thresholds, the national health and nutrition examination survey 1999–2002. Hear Res 2018;358:30–36. - PubMed
-
- Gordon-Salant S Hearing loss and aging: new research findings and clinical implications. J Rehabil Res Dev 2005;42(suppl 2):9–24. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
