

Urinary apolipoprotein A4 as a biomarker for renal allograft injury in kidney transplant recipients
- PMID: 40397923
- PMCID: PMC12094748
- DOI: 10.1371/journal.pone.0324529
Urinary apolipoprotein A4 as a biomarker for renal allograft injury in kidney transplant recipients
Abstract
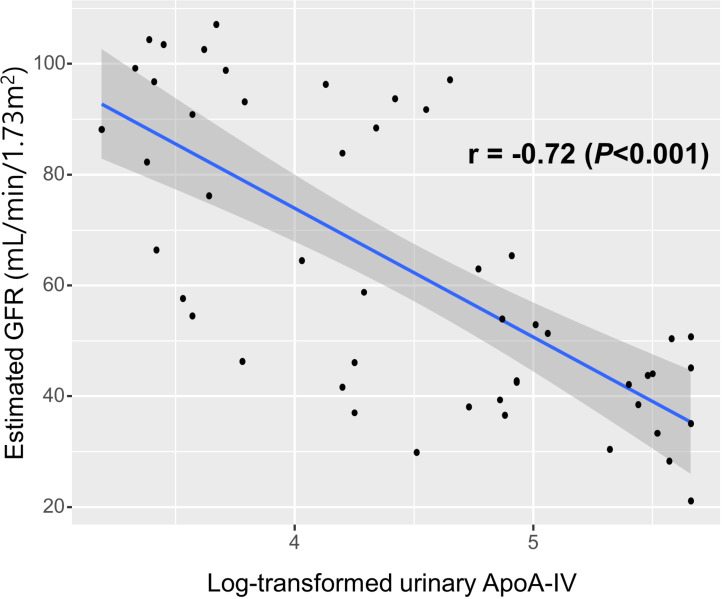
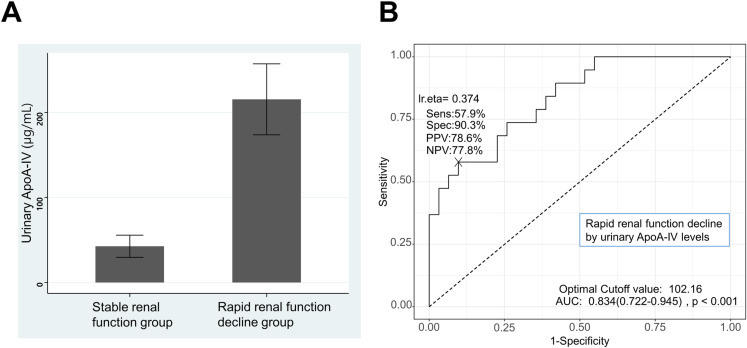
Chronic renal allograft injury (CRAI) is a major cause of allograft loss in kidney transplant recipients (KTRs). The aim of this study was to evaluate the associations of urinary apolipoprotein A4 (ApoA-IV) levels with renal function and rapid renal function decline in KTRs. This study included 50 KTRs. Proteomic analysis via liquid chromatography‒mass spectrometry and tandem mass spectrometry (LC-MS/MS) was performed to identify potential urinary biomarkers. The SWATH (sequential window acquisition of all theoretical mass spectra) method was used for protein quantification. Urinary ApoA-IV levels were validated by enzyme-linked immunosorbent assay (ELISA). Rapid renal function decline was defined as an estimated glomerular filtration rate (GFR) decrease of >3 mL/min/1.73 m2 per year or initiation of dialysis. The log-transformed urinary ApoA-IV levels measured by ELISA had a significantly inverse correlation with the estimated GFR (r = -0.72, P < 0.001). Moreover, urinary ApoA-IV levels were higher in patients with rapid renal function decline than in those with stable renal function (215.4 ± 181.8 μg/mL vs. 42.5 ± 72.4 μg/mL, P = 0.001). Univariate logistic regression analysis revealed that log-transformed urinary ApoA-IV levels were significantly associated with rapid renal function decline (odds ratio [OR] 6.70, 95% confidence interval [CI] 2.56-22.83; P < 0.001). Multiple logistic regression showed urinary ApoA-IV levels remained a significant risk factor for rapid renal function decline (OR 4.10, 95% CI 1.10-19.55; P = 0.047). ROC curve analysis revealed the area under the curve (AUC) of 0.834 (95% CI 0.722-0.945, P < 0.001) for urinary ApoA-IV levels in predicting rapid renal function decline. Our results suggest that urinary ApoA-IV levels might be a potential biomarker for renal allograft function and could be used as a predictor for rapid renal function decline in KTRs.
Copyright: © 2025 Kee et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Urinary Retinol-Binding Protein 4 is Associated With Renal Function and Rapid Renal Function Decline in Kidney Transplant Recipients.Transplant Proc. 2022 Mar;54(2):362-366. doi: 10.1016/j.transproceed.2021.10.028. Epub 2022 Jan 28. Transplant Proc. 2022. PMID: 35094884
-
High Urinary Aspartate Aminotransferase in the Late Posttransplant Period Predicts Rapid, Progressive Decline in Kidney Allograft Function.Exp Clin Transplant. 2017 Jun;15(3):267-276. doi: 10.6002/ect.2016.0081. Epub 2017 Mar 22. Exp Clin Transplant. 2017. PMID: 28332956
-
Blood Pressure, Chronic Kidney Disease Progression, and Kidney Allograft Failure in Kidney Transplant Recipients: A Secondary Analysis of the FAVORIT Trial.Am J Hypertens. 2019 Aug 14;32(9):816-823. doi: 10.1093/ajh/hpz095. Am J Hypertens. 2019. PMID: 31179500 Free PMC article.
-
High urinary interleukin-2 in late post-transplant period portends a risk of decline in kidney allograft function: a preliminary study.BMC Res Notes. 2017 Nov 21;10(1):605. doi: 10.1186/s13104-017-2936-7. BMC Res Notes. 2017. PMID: 29162160 Free PMC article.
-
Urinary calprotectin and posttransplant renal allograft injury.PLoS One. 2014 Nov 17;9(11):e113006. doi: 10.1371/journal.pone.0113006. eCollection 2014. PLoS One. 2014. PMID: 25402277 Free PMC article.
References
-
- Ganji MR, Harririan A. Chronic allograft dysfunction: major contributing factors. Iran J Kidney Dis. 2012;6(2):88–93. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
