

Does the IL-6/KL-6 ratio distinguish different phenotypes in COVID-19 Acute Respiratory Distress Syndrome? An observational study stemmed from prospectively derived clinical, biological, and computed tomographic data
- PMID: 40397955
- PMCID: PMC12094726
- DOI: 10.1371/journal.pone.0321533
Does the IL-6/KL-6 ratio distinguish different phenotypes in COVID-19 Acute Respiratory Distress Syndrome? An observational study stemmed from prospectively derived clinical, biological, and computed tomographic data
Abstract
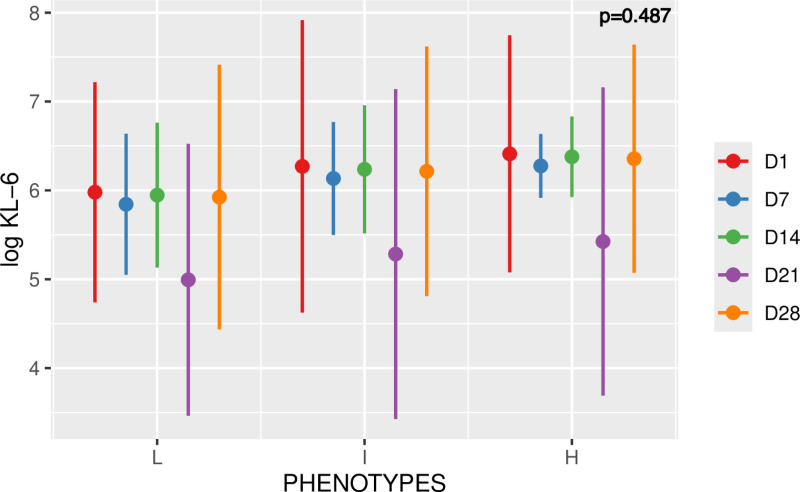
Background: As new SARS-CoV-2 variants emerge and as treatment of COVID-19 ARDS remains exclusively supportive, there is an unmet need to better characterize its different phenotypes to tailor personalized treatments. Clinical, biological, spirometric and CT data hardly allow deciphering of Heavy (H), Intermediate (I) and Light (L) phenotypes of COVID-19 ARDS and the implementation of tailored specific strategies (prone positioning, PEEP settings, recruitment maneuvers). We hypothesized that the ratio of two pivotal COVID-19 biomarkers (interleukin 6 [IL-6] and Krebs von den Lungen 6 [KL-6], related to inflammation and pneumocyte repair, respectively) would provide a biologic insight into the disease timeline allowing 1) to differentiate H, I and L phenotypes, 2) to predict outcome and 3) to reflect some of CT findings.
Methods and findings: This was a retrospective analysis of prospectively acquired data (COVID HUS cohort). Inclusion concerned any patient with severe COVID-19 pneumonia admitted to two intensive care units between March 1st and May 1st, 2020, in a high-density cluster of the first epidemic wave (Strasbourg University Hospital, France). Demographic, clinical, biological (standard, IL-6 [new generation ELISA], KL-6 [CLEIA technique]), spirometric (driving pressure, respiratory system compliance) and CT data were collected longitudinally. CT analysis included semi-automatic and automatic lung measurements and allowed segmentation of lung volumes into 4 (poorly aerated, non-aerated, overinflated and normally aerated) and 3 (ground-glass, restricted normally aerated, and overinflated) zones, respectively. The primary outcome was to challenge the IL-6/KL-6 ratio capacity to decipher the three COVID-19 ARDS phenotypes (H, I and L) defined on clinical, spirometric and radiologic grounds. Secondary outcomes were the analysis of the prognostic value of the IL-6/KL-6 ratio and its correlates with CT-acquired data. Multivariate analysis was based on principal component analysis. One hundred and forty-eight ventilated COVID-19 ICU patients from the COVID HUS cohort were assessed for eligibility and 77 were included in the full analysis. Most were male, all were under invasive mechanical ventilation and vasopressor therapy and displayed high severity scores (SAPSII: 48 [42-56]; SOFA: 8 [7-10]). The L, I and H COVID ARDS phenotypes were identified in 11, 15 and 48 patients, respectively. In three patients, the phenotype could not be defined precisely. Thirty patients (39%) died in the ICU and the number of ventilator-free days was 2 [0-2] days. The IL-6/KL-6 ratio was not significantly different between the L, I and H phenotypes and evolved according to similar patterns over time. Surviving and deceased patients displayed an inverse kinetic of KL-6. IL-6 and the IL-6/KL-6 ratio were linearly associated with ground-glass volume on semi-automatic and automatic CT lung measurements.
Conclusions: In our population of severe ventilated COVID ARDS patients, the IL-6/KL-6 ratio was not clue to differentiate the H, I and L phenotypes and tailor a personalized ventilatory approach. There was an interesting correlation between IL-6/KL-6 ratio and ground-glass volume as determined by automated lung CT analysis. Such correlation deserves more in-depth pathophysiological study, at best gathered from a prospective cohort with a larger sample size and histological analysis.
Trial registration: COVID HUS Trial registration number: NCT04405726.
Copyright: © 2025 Partouche et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
Eric Noll shares a patent related to lung segmentation: “Automatic determination method of at least one parameter indicative of the degree or level of functionality of a lung” WO2021209542A1, US20230298164A1 This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures








References
-
- WHO. Coronavirus (COVID-19) dashboard > deaths. https://data.who.int/dashboards/covid19/deaths.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
