

A machine learning based prediction model for short term efficacy of nasopharyngeal carcinoma
- PMID: 40399535
- PMCID: PMC12095505
- DOI: 10.1038/s41598-025-02897-w
A machine learning based prediction model for short term efficacy of nasopharyngeal carcinoma
Abstract
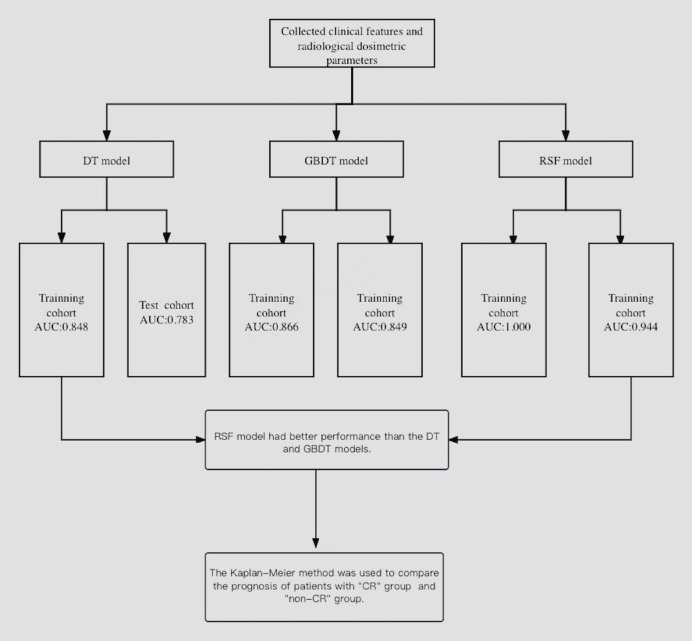
The radiological dosimetric parameters and clinical features were screened by machine learning to construct a prediction model for the short-term efficacy of locally advanced Nasopharyngeal Carcinoma (LANPC). Patients diagnosed with Nasopharyngeal Carcinoma were retrospectively collected in the study. Twenty-four clinical features and twelve radiological dosimetric features were included. Three machine learning algorithms were used to construct predictive models for the short-term efficacy of LANPC. Kaplan-Meier log-rank method was used to compare the prognosis of patients with different efficacies in the model. The reliability of the model was evaluated using the calibration curve and the area under the curve (AUC). There were 194 patients who met the inclusion criteria. Among the three models being constructed, Random forest (RSF) model showed the best predictive ability, with AUC values of 1.000 in the training group and 0.944 in the test group, followed by XGBoost decision tree (GBDT) model (0.866/0.849) and decision tree (DT) model (0.848/0.783). In RSF model, the 3-year and 5-year overall survival rates of patients in complete remission (CR) group were 98.9% (95% CI 0.9688-1.0000) and 89.7% (95% CI 0.8256-0.9752), respectively.While for patients in non-CR group, the 3-year and 5-year overall survival (OS) rate was 100% (95%CI 1.000~1.000) and 98.8% (95% CI 0.9652-1.0000), respectively. There has statistically significant difference between the two groups (P = 0.0037). RSF model constructed by machine-learning algorithm based on radiological dosimetric parameters and clinical characteristics can better predict the short-term efficacy of LANPC, and is an effective tool to evaluate the short-term efficacy of different LANPC patients during treatment.
Keywords: Locoregionally advanced nasopharyngeal carcinoma; Machine-learning algorithm; Radiological dosimetric parameters; Short-term efficacy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: The study was approved by the Ethics Committee of the Second Affiliated Hospital of Guangxi Medical University. The requirement for informed consent was waived by the ethics committee/Institutional Review Board of the Second affiliated Hospital of Guangxi Medical University. All methods were performed in accordance with the relevant guidelines and regulations. Consent for publication: Not applicable.
Figures





Similar articles
-
Comparative evaluation of machine learning models in predicting overall survival for nasopharyngeal carcinoma using 18F-FDG PET-CT parameters.Clin Transl Oncol. 2025 Apr;27(4):1748-1759. doi: 10.1007/s12094-024-03709-9. Epub 2024 Sep 20. Clin Transl Oncol. 2025. PMID: 39304599
-
MRI-based random survival Forest model improves prediction of progression-free survival to induction chemotherapy plus concurrent Chemoradiotherapy in Locoregionally Advanced nasopharyngeal carcinoma.BMC Cancer. 2022 Jul 6;22(1):739. doi: 10.1186/s12885-022-09832-6. BMC Cancer. 2022. PMID: 35794590 Free PMC article.
-
Guiding induction chemotherapy of locoregionally advanced nasopharyngeal carcinoma with ternary classification of predicted individual treatment effect.Radiother Oncol. 2024 Dec;201:110571. doi: 10.1016/j.radonc.2024.110571. Epub 2024 Oct 10. Radiother Oncol. 2024. PMID: 39393470
-
Using machine learning algorithms to predict the prognosis of advanced nasopharyngeal carcinoma after intensity-modulated radiotherapy.Curr Probl Cancer. 2024 Feb;48:101040. doi: 10.1016/j.currproblcancer.2023.101040. Epub 2023 Nov 16. Curr Probl Cancer. 2024. PMID: 37979476 Review.
-
Advances and challenges in immunotherapy for locally advanced nasopharyngeal carcinoma.Cancer Treat Rev. 2024 Dec;131:102840. doi: 10.1016/j.ctrv.2024.102840. Epub 2024 Oct 11. Cancer Treat Rev. 2024. PMID: 39426201 Review.
References
-
- Tian, Y. M. et al. Long-term outcome and pattern of failure for patients with nasopharyngeal carcinoma treated with intensity-modulated radiotherapy. Head Neck. 41 (5), 1246–1252. 10.1002/hed.25545 (2019). - PubMed
-
- Sun, Y. et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: a phase 3, multicentre, randomised controlled trial. Lancet Oncol.17 (11), 1509–1520. 10.1016/S1470-2045(16)30410-7 (2016). - PubMed
-
- Chen, Y. P. et al. Chemotherapy in combination with radiotherapy for Definitive-Intent treatment of stage II-IVA nasopharyngeal carcinoma: CSCO and ASCO guideline. J. Clin. Oncol.39 (7), 840–859. 10.1200/JCO.20.03237 (2021). - PubMed
-
- Pfister, D. G. et al. Head and neck cancers, version 2.2020, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Canc Netw.18 (7), 873–898. 10.6004/jnccn.2020.0031 (2020). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
