

Cardiovascular risk profile in subjects with diabetes: Is SCORE2-Diabetes reliable?
- PMID: 40399956
- PMCID: PMC12096474
- DOI: 10.1186/s12933-025-02769-7
Cardiovascular risk profile in subjects with diabetes: Is SCORE2-Diabetes reliable?
Abstract
Background: People living with type 2 diabetes (T2D) are at a two- to four-fold higher risk of developing cardiovascular disease (CVD) compared with those without T2D, making early assessment of their CV risk essential. European Society of Cardiology (ESC) has developed a new model to estimate 10-year CV risk in people with T2D aged ≥ 40 years: SCORE2-Diabetes. Despite its advantages, several aspects remain to be clarified. This study evaluated the association between CV risk stratified by SCORE2-Diabetes and early CV damage assessed through arterial stiffness, intima-media thickness (IMT), and carotid atherosclerosis. Additionally, it examined the agreement between risk stratification by SCORE2 and SCORE2-Diabetes and their concordance with vascular damage.
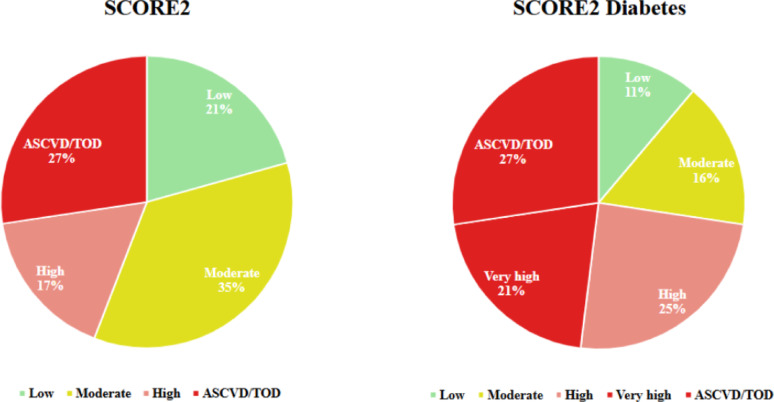
Methods: Pulse wave velocity (PWV), IMT, and carotid atherosclerosis were assessed in 179 individuals with T2D aged 40-69 years, categorized into SCORE2-Diabetes risk groups: Low (n = 20), Moderate (n = 29), High (n = 44), and very high (n = 37). Patients with a history of atherosclerotic cardiovascular disease (ASCVD) or severe target organ damage (TOD) constituted another group (ASCVD/TOD, n = 49).
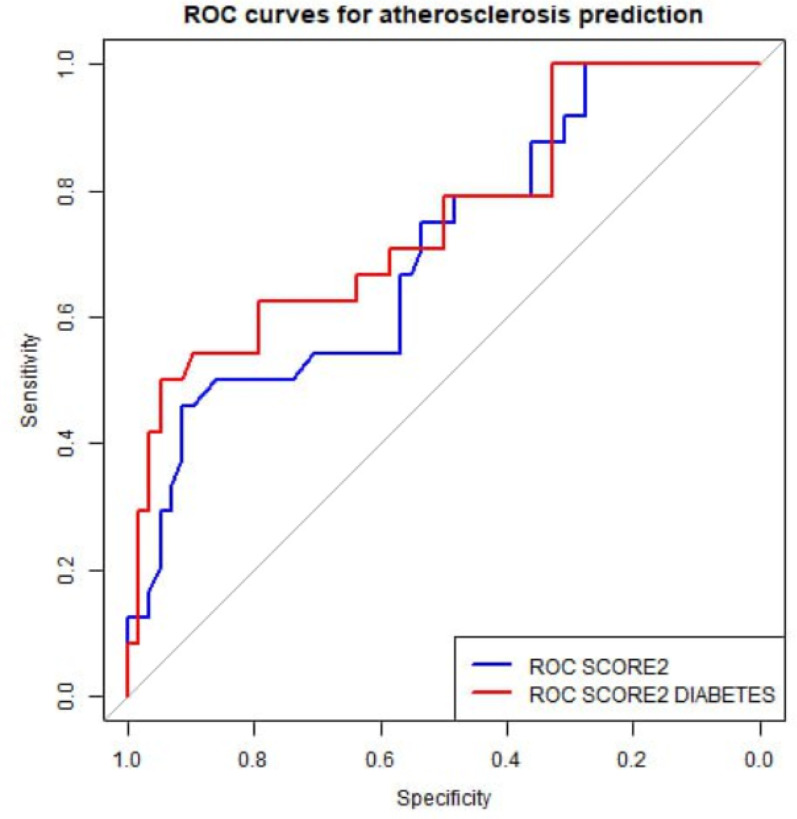
Results: PWV was significantly increased from Low to very high and ASCVD/TOD groups (7.2 ± 1.1, 8.7 ± 1.9, 9.8 ± 2.3, 12.8 ± 5.1 and 11.5 ± 3.8 m/s, respectively). Similarly, IMT showed a stepwise increase with risk class (0.68 ± 0.11, 0.78 ± 0.13, 0.83 ± 0.12, 0.86 ± 0.19 and 0.87 ± 0.15 mm, respectively). Patients in very high or ASCVD/TOD group showed a higher prevalence of carotid atherosclerosis than other groups (0%, 17.24%, 11.40%, 37.83% and 40.81%, respectively). No significant differences were found between the very high and ASCVD/TOD groups in any parameter. The correlation between PWV values and increasing CV risk was stronger for SCORE2-Diabetes than for SCORE2. ROC curve analysis showed SCORE2-Diabetes had superior predictive performance for carotid atherosclerosis and high PWV compared to SCORE2 (p = 0.048).
Conclusions: Higher PWV, IMT, and carotid atherosclerosis prevalence were associated with increasing CV risk stratified by SCORE2-Diabetes, with no significant differences between the very high and ASCVD/TOD groups. SCORE2-Diabetes demonstrated a better identification of preclinical vascular damage compared to SCORE2, supporting its use as a reliable tool for identifying vascular damage in T2D patients without ASCVD or TOD.
Keywords: Arterial stiffness; Atherosclerosis; Cardiovascular risk; Intima-media thickness; SCORE2-Diabetes; Type 2 diabetes.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Comitato Etico Catania 2, protocol n. 270/C.E. 26th April 2022. Informed consent was obtained from every participant. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures




References
-
- Timmis A, Vardas P, Townsend N, Torbica A, Katus H, De Smedt D, et al. European society of cardiology: cardiovascular disease statistics 2021. Eur Heart J. 2022;43(8):716–99. - PubMed
-
- Goff DC, Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation [Internet]. 2014 Jun 24 [cited 2025 Mar 3];129(25_suppl_2). Available from: https://www.ahajournals.org/doi/10.1161/01.cir.0000437741.48606.98
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
