

Cerebral perfusion pressure targets after traumatic brain injury: a reappraisal
- PMID: 40399968
- PMCID: PMC12096506
- DOI: 10.1186/s13054-025-05458-9
Cerebral perfusion pressure targets after traumatic brain injury: a reappraisal
Abstract
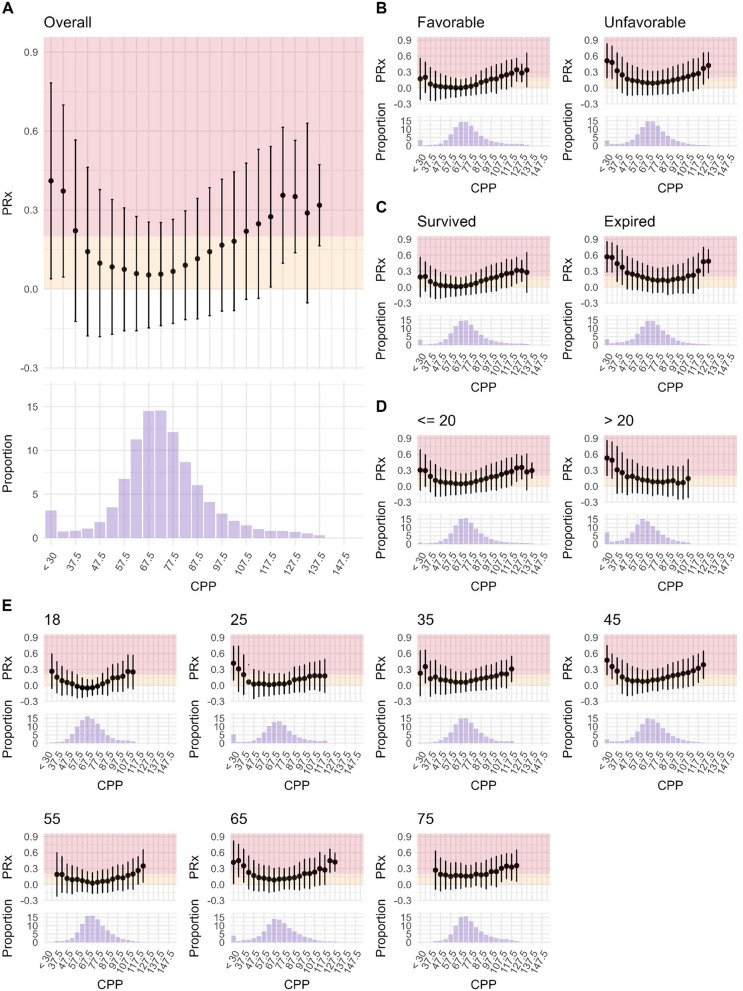
Introduction: Cerebral perfusion pressure (CPP) management is central to neurocritical care management after traumatic brain injury (TBI). While the Brain Trauma Foundation recommends a target of 60-70 mmHg, it is unclear whether this range reflects the lower limit or the optimal level, when viewed through the prism of cerebrovascular autoregulation. Autoregulation aims at stabilizing cerebral blood flow and can be estimated continuously using the pressure reactivity index (PRx). Personalized CPP targets can be derived from PRx including CPPopt (optimal CPP), LLA, and ULA (lower and upper limit of autoregulation). Emerging data suggests an asymmetric relationship around CPPopt, with more pronounced autoregulation deterioration with decreasing compared to increasing CPP. Based on the hypothesis that higher CPP levels may be less harmful than lower CPP levels, we aimed to reassess rigorously the prognostic value of the different CPP targets.
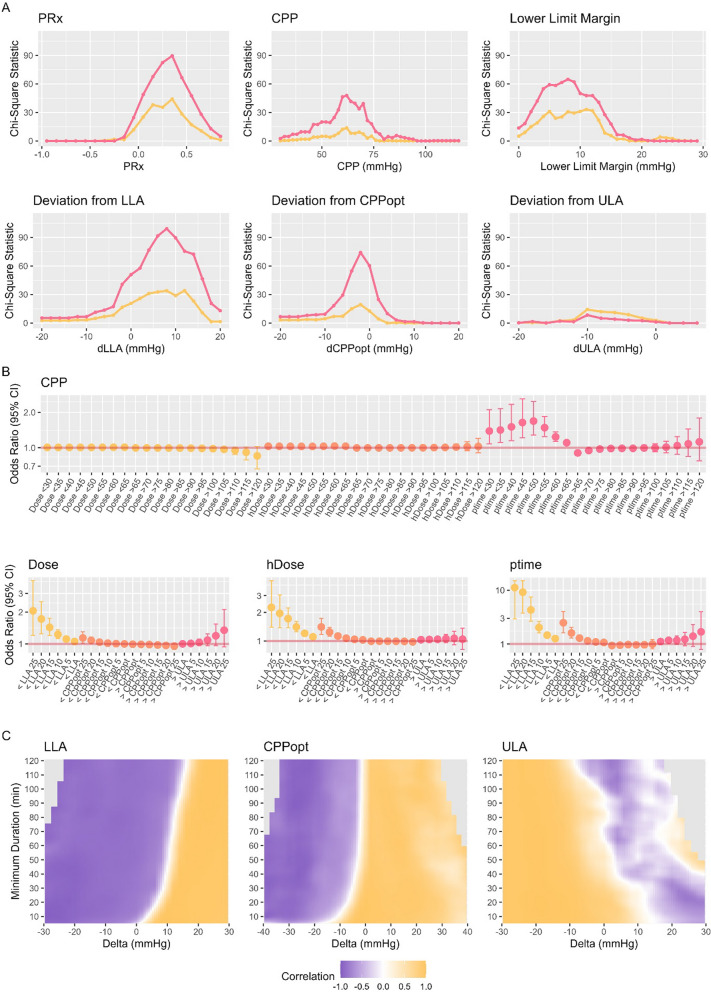
Material and methods: We analyzed 809 adult TBI patients admitted from 2002 to 2023 who underwent invasive intracranial pressure monitoring and had available 6-month outcomes. CPPopt, LLA, and ULA were estimated using previously published methodologies. Deviations of CPP from fixed or personalized targets were assessed describing the overall dose, the hourly dose and the percentage time spent outside of these targets and examined using Chi-squared tests, logistic regressions, heatmaps, ordinal analyses, and group-based trajectory modelling.
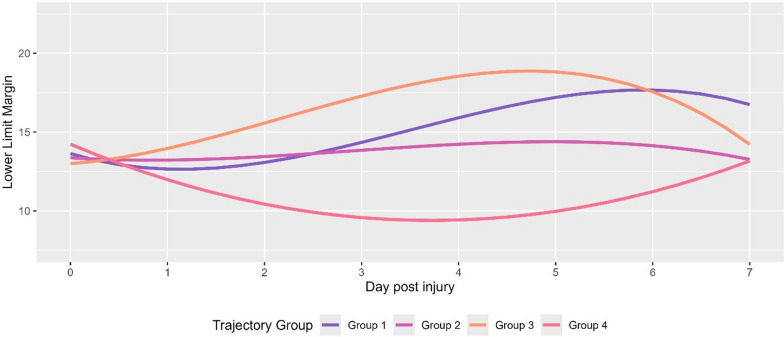
Results: Our data confirms an asymmetric CPP/PRx relationship with steeper increases in PRx with decreasing and only modest elevations with increasing CPP. Even small decreases below CPPopt were consistently linked to worse outcomes (OR 1.04 (CI 1.02-1.06) and 1.09 (CI 1.04-1.15) for hourly dose and percentage time spent below CPPopt, p < 0.001 and p = 0.001 respectively). The strength of association increased with further decreases in CPP away from CPPopt towards the LLA with OR of 1.11 (CI 1.07-1.14) and 1.26 (CI 1.18-1.35) for hourly dose and percentage time spent below LLA respectively (p < 0.001). Conversely, higher-than CPPopt levels generally showed no association to worse outcomes. Distinct trajectories in the relationship between CPPopt and LLA (introduced as the Lower Limit Margin) could be identified with worse outcomes in those with decreasing distance between these targets (Mortality of 18% vs. 45% for patients with increasing vs. decreasing lower limit margins, p = 0.003).
Conclusion: Our findings corroborate experimental work suggesting that TBI patients are more vulnerable to CPP reductions below as compared to elevations above personalized thresholds. The results highlight the need for individualized CPP management strategies that prioritize avoidance of lower CPP levels and suggest using CPPopt as the lower CPP limit.
Keywords: Blood pressure targets; Cerebral perfusion pressure; Cerebrovascular autoregulation; Multimodality monitoring; Traumatic brain injury.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval and consent to participate: The data was accessed through the Brain Physics database that is approved by the local ethics committee (REC 23/YH/0085). Informed consent was waived by the local ethics committee. Consent to publish: Not applicable. Competing interest: ICM + is a software licensed by Cambridge Enterprise Ltd. PS has a financial interest in a part of licensing fee; the licensing fee was waived for this study.
Figures
Comment in
-
Reconsidering the symmetric assumption in CPP-PRx modeling for traumatic brain injury.Crit Care. 2025 Jul 14;29(1):304. doi: 10.1186/s13054-025-05551-z. Crit Care. 2025. PMID: 40660359 Free PMC article. No abstract available.
References
-
- Carney N, Totten AM, O’Reilly C, et al. Guidelines for the management of severe traumatic brain injury. Neurosurgery. 2017;80(1):6–15. - PubMed
-
- Patel PM, Drummond JC, Lemkuil B. Miller’s anesthesia. Elsevier Saunders; 2014.
-
- Czosnyka M, Smielewski P, Kirkpatrick P, Laing RJ, Menon D, Pickard JD. Continuous assessment of the cerebral vasomotor reactivity in head injury. Neurosurgery. 1997;41(1):11–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
