

Association of myeloid cell reactivity patterns with safe food predictions in FPIES patients
- PMID: 40400028
- PMCID: PMC12093898
- DOI: 10.1186/s13223-025-00968-1
Association of myeloid cell reactivity patterns with safe food predictions in FPIES patients
Abstract
Background: Food protein-induced enterocolitis syndrome (FPIES) is an understudied non-IgE-mediated food allergy, which is distinct from and lacks diagnostic testing akin to IgE testing. FPIES affects infants and toddlers but can persist into adulthood. As there are no extant methods to identify safe foods for FPIES patients, food ingestion trials are performed at home and often lead to reactions and development of food aversions, which may lead to failure-to-thrive and gastric feeding tube requirements. We hypothesized that foods that fail to elicit responses in immune cells of FPIES patients would be safe to ingest, which could support development of a diagnostic method to headstart safe food identification in patients.
Methods: We developed an ex vivo model of FPIES using food-stimulated white blood cells (WBCs) from pediatric FPIES patients and controls by defining a 9-gene panel representative of FPIES ex vivo responses and conducted a single-arm pilot clinical trial.
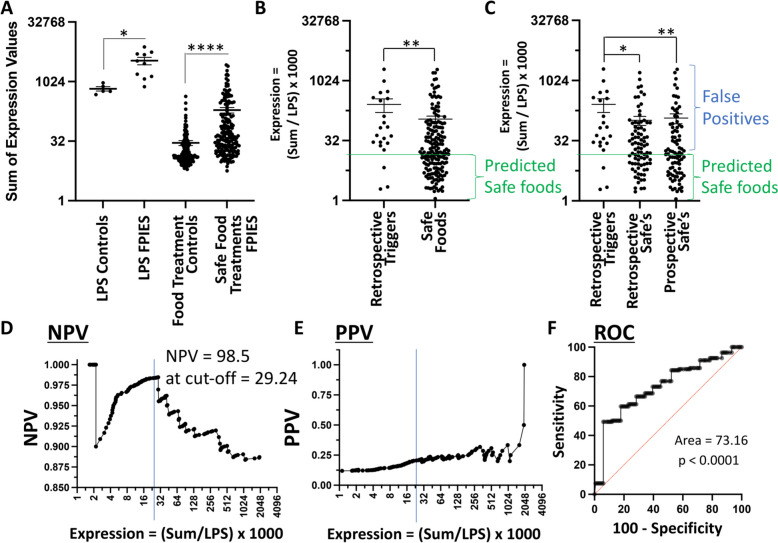
Results: Myeloid cells of FPIES patients displayed variable individual-specific myeloid cell reactivity patterns (iMCRPs) to different foods. Foods that failed to elicit repsonses in patients' immune cells were safe to ingest with a negative predictive value of 98.5%. This, when utilized in prospective predictions, reduced newly introduced food reaction rates from 19.5 to 0% while increasing food repertoire diversity.
Conclusions: iMCRPs represent a novel and potentially useful tool that associates with safe food ingestion in FPIES patients for foods that fail to elicit immune cell reactions. Trial Registration The trial has been registered at registered at ClinicalTrials.gov # NCT04644783.
Keywords: Diarrhea; FPIES; Food allergy; Gastrointestinal inflammation; Non-IgE food allergy; Vomiting.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Institutional Review Board (IRB) at the University of Michigan under IRB protocol # HUM00156027. Written informed consent was signed for by one one of the participants’ parents or guardians. Recruitment of FPIES participants was conducted under a single-arm clinical trial of 10 FPIES participants, registered at ClinicalTrials.gov (NCT04644783). Blood samples from 5 de-identified non-FPIES participants were collected independently of the clinical trial, serving as an external control arm under IRB protocol #HUM00208717. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Nowak-Wegrzyn A, Chehade M, Groetch ME, Spergel JM, Wood RA, Allen K, et al. International consensus guidelines for the diagnosis and management of food protein-induced enterocolitis syndrome: executive summary-workgroup report of the adverse reactions to foods committee, American academy of allergy, asthma & immunology. J Allergy Clin Immunol. 2017;139(4):1111-26 e4. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
