

Multiple myeloma care, treatment patterns, and treatment durations in academic and community care settings
- PMID: 40400295
- PMCID: PMC12150631
- DOI: 10.1080/14796694.2025.2504318
Multiple myeloma care, treatment patterns, and treatment durations in academic and community care settings
Abstract
Aim: Evaluate multiple myeloma (MM) treatment patterns, healthcare utilization (HCRU), and costs from academic and community settings.
Methods: This observational study linked US MM insurance claims (1 April 2017-30 June 2022) with provider affiliations to evaluate patient characteristics and treatment durations across patient cohorts defined by care setting of treatment (academic only, community only, mixed [both]), as well as treatment patterns, HCRU, and costs of care (e.g. treatment, office visits, hospitalization) in each setting.
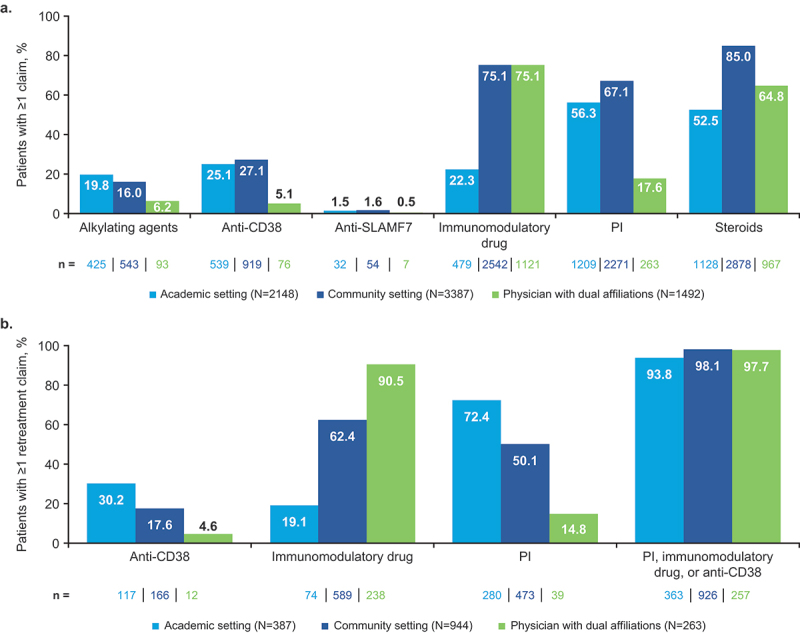
Results: 3778 patients were included. By cohort (n = 530 academic; n = 1647 community), the community cohort was older with more comorbidities. Mixed-cohort patients (n = 1601) frequently initiated treatment at community centers and briefly shifted to academic centers for transplant. Among 3778 patients who received MM-related care, most claims were from the community setting. The academic setting had high rates of claims for proteasome inhibitors (56.3% of patients) and steroids (52.5%); the community setting had high rates for immunomodulatory drugs (75.1%) and steroids (85.0%). Stem cell transplant claims were more common for academic versus community (21.4%/7.3%). Treatment duration/time to next therapy were similar between cohorts. Costs were generally higher in the academic versus community settings.
Conclusion: Improved patient support is needed in community settings, where most MM care occurs.
Keywords: Hematologic/myeloma; outcomes research; real-world evidence; treatment patterns.
Plain language summary
Patients with a type of blood cancer called multiple myeloma (MM) face complex treatment journeys, and most patients require multiple treatments over time to control the disease. Patients can receive treatments in different care settings. An academic setting includes hospitals/healthcare centers that train doctors and medical students. A community setting includes non-academic hospitals and centers. To access different treatments, patients with MM often receive care in both settings. Research has shown that patients treated in academic settings tend to live longer than patients treated in community settings, but more research is needed to understand the reasons for this difference. The goal of this study was to determine if there were differences between patients who received MM treatments in academic versus community settings, examine the types of MM treatments given, the services received, and the costs in each setting. We found that patients received most of their MM care in the community setting. Patients who received all their MM treatments in a community setting were older, more likely to have multiple health complications, and less likely to participate in clinical trials. A specialized treatment called a stem cell transplant was more frequently given in the academic setting, and patients often moved between settings to receive this treatment. In both settings, patients were often treated with the same drug more than once, which could reduce its effectiveness. Costs overall were higher in the academic setting. These findings show a need for new treatments that are available in both academic and community settings.
Conflict of interest statement
Natalie Boytsov is an employee of and holds financial equities in GSK; Catherine B. McGuiness is an employee of IQVIA; Zifan Zhou is an employee of IQVIA; Tianyao Huo is an employee of IQVIA; Kathleen Montgomery is an employee of and holds financial equities in GSK; Nirali Kotowsky is a former employee of and held financial equities in GSK; Chi-Chang Chen is an employee of IQVIA. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures




Similar articles
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Antidepressants for pain management in adults with chronic pain: a network meta-analysis.Health Technol Assess. 2024 Oct;28(62):1-155. doi: 10.3310/MKRT2948. Health Technol Assess. 2024. PMID: 39367772 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
Cited by
-
Impact of social determinants of health on treatment patterns and outcomes in multiple myeloma.Future Oncol. 2025 Jun;21(13):1663-1673. doi: 10.1080/14796694.2025.2498878. Epub 2025 May 12. Future Oncol. 2025. PMID: 40351131 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous