

Margins in oncologic nasopharyngeal surgery: a systematic review with meta-analysis
- PMID: 40400377
- PMCID: PMC12115408
- DOI: 10.14639/0392-100X-suppl.1-45-2025-N1170
Margins in oncologic nasopharyngeal surgery: a systematic review with meta-analysis
Abstract
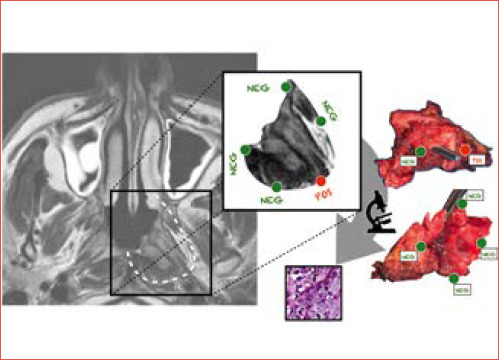
Objective: Nasopharyngeal malignancies are rare heterogenous histologies (nasopharyngeal carcinoma [NPC], minor salivary glands carcinomas, and low-grade papillary nasopharyngeal adenocarcinoma) and a significant proportion of patients experience loco-regional recurrence after primary treatment. Resection margin status is a key prognostic factor that influences recurrence and survival, although definitions and criteria for negative, close, and positive margins remain inconsistent. This systematic review with meta-analysis aimed to summarise the existing definitions of resection margins in the literature and evaluate their impact on clinical outcomes in patients undergoing nasopharyngectomy with a specific focus on NPC.
Methods: A systematic literature review was conducted according to PRISMA guidelines. Electronic databases (Scopus, PubMed, and Web of Science) were searched up to November 2024. Studies reporting on surgical margins and survival outcomes in patients with NPC treated with endoscopic or open nasopharyngectomy were included. Pooled odds ratios (OR) for overall survival (OS), disease-specific survival (DSS), and disease-free survival (DFS) were calculated using a random-effects model.
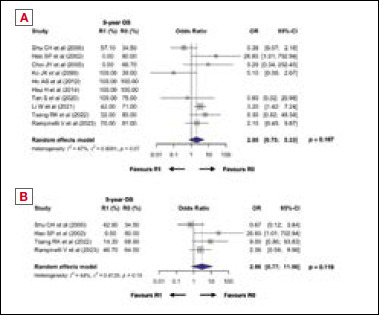
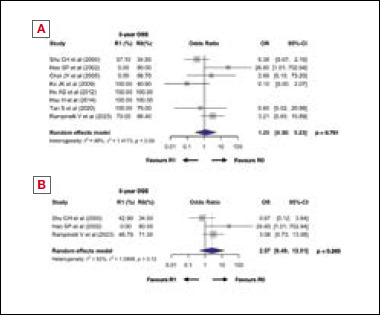
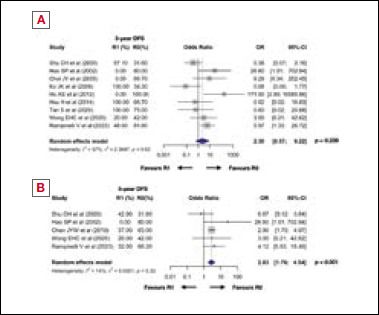
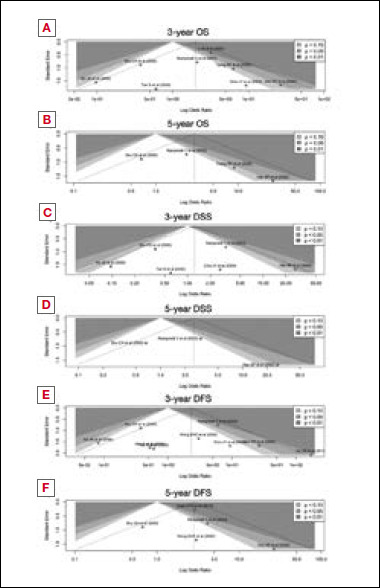
Results: A total of 45 studies met the inclusion criteria, with 12 included in the meta-analysis. Positive surgical margins were associated with worse 5-year DFS (OR 2.21, 95% CI 1.55-3.14, p < 0.001), while no significant impact was observed on 3-year DFS (OR 2.3, p = 0.239), 3-year OS (OR 2, p = 0.167), 5-year OS (OR 2.98, p = 0.115), 3-year DSS (OR 1.25, p = 0.761), or 5-year DSS (OR 2.57, p = 0.265). Margin positivity rates were 16.9% for endoscopically-treated NPC, 20.6% for open-surgery NPC, and 20.6% for mixed histology, with no significant difference between surgical approaches (p = 0.995).
Conclusions: Positive resection margins significantly impact DFS in recurrent NPC. Standardised margin definitions are needed to improve prognostication and guide decisions on adjuvant therapy.
Keywords: endoscopic surgery; nasopharyngeal cancer; nasopharyngectomy; surgical margin; survival outcome.
Copyright © 2025 Società Italiana di Otorinolaringoiatria e Chirurgia Cervico-Facciale, Rome, Italy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
The impact of resection margins in hypopharyngeal surgery: a systematic review and meta-analysis.Acta Otorhinolaryngol Ital. 2025 May;45(Suppl. 1):S99-S108. doi: 10.14639/0392-100X-suppl.1-45-2025-N1078. Acta Otorhinolaryngol Ital. 2025. PMID: 40400380 Free PMC article.
-
Prognostic significance of surgical margins in open neck horizontal laryngectomy: a systematic review and meta-analysis.Acta Otorhinolaryngol Ital. 2025 May;45(Suppl. 1):S87-S98. doi: 10.14639/0392-100X-suppl.1-45-2025-N992. Acta Otorhinolaryngol Ital. 2025. PMID: 40400379 Free PMC article.
-
Endoscopic nasopharyngectomy in recurrent nasopharyngeal carcinoma: a case series, literature review, and pooled analysis.Int Forum Allergy Rhinol. 2017 Apr;7(4):425-432. doi: 10.1002/alr.21881. Epub 2016 Nov 16. Int Forum Allergy Rhinol. 2017. PMID: 27865062
-
Salvage surgery in nasopharyngeal Cancer: Unraveling the efficacy of transnasal endoscopic nasopharyngectomy for advanced stage recurrent tumors.Oral Oncol. 2024 Dec;159:107048. doi: 10.1016/j.oraloncology.2024.107048. Epub 2024 Oct 2. Oral Oncol. 2024. PMID: 39362026
-
Pretreatment hematologic markers as prognostic factors in patients with nasopharyngeal carcinoma: A systematic review and meta-analysis.Medicine (Baltimore). 2017 Mar;96(11):e6364. doi: 10.1097/MD.0000000000006364. Medicine (Baltimore). 2017. PMID: 28296774 Free PMC article.
References
-
- Bray F, Ferlay J, Soerjomataram I, et al. . Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394-424. https://doi.org/10.3322/caac.21492 10.3322/caac.21492 - DOI - PubMed
-
- Badoual C. Update from the 5th edition of the World Health Organization Classification of Head and Neck Tumors: oropharynx and nasopharynx. Head Neck Pathol 2022;16:19-30. https://doi.org/10.1007/s12105-022-01449-2 10.1007/s12105-022-01449-2 - DOI - PMC - PubMed
-
- Liu J, Yu H, Sun X, et al. . Salvage endoscopic nasopharyngectomy for local recurrent or residual nasopharyngeal carcinoma: a 10-year experience. Int J Clin Oncol 2017;22:834-842. https://doi.org/10.1007/s10147-017-1143-9 10.1007/s10147-017-1143-9 - DOI - PubMed
-
- Chen Y-P, Chan ATC, Le Q-T, et al. . Nasopharyngeal carcinoma. Lancet 2019;394:64-80. https://doi.org/10.1016/S0140-6736(19)30956-0 10.1016/S0140-6736(19)30956-0 - DOI - PubMed
-
- Chee J, Ting Y, Ong YK, et al. . Relapse status as a prognostic factor in patients receiving salvage surgery for recurrent or residual nasopharyngeal cancer after definitive treatment. Head Neck 2016;38:1393-1400. https://doi.org/10.1002/hed.24451 10.1002/hed.24451 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
