

Efficacy and Safety of a Continuous Intravenous Insulin Protocol Modified for East Asians in Postoperative Glycemic Management Following Pancreatectomy
- PMID: 40400655
- PMCID: PMC12094835
- DOI: 10.7759/cureus.84527
Efficacy and Safety of a Continuous Intravenous Insulin Protocol Modified for East Asians in Postoperative Glycemic Management Following Pancreatectomy
Abstract
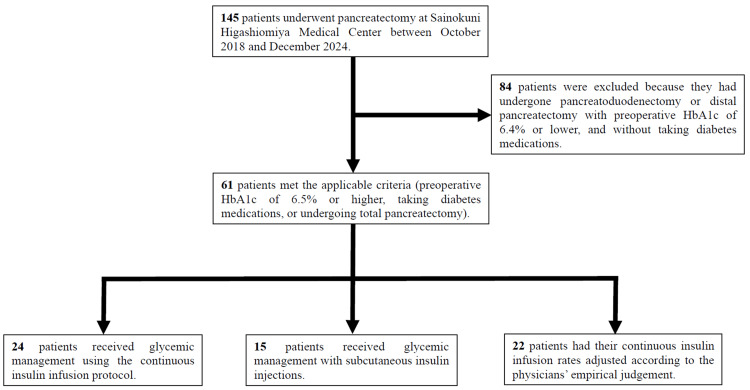
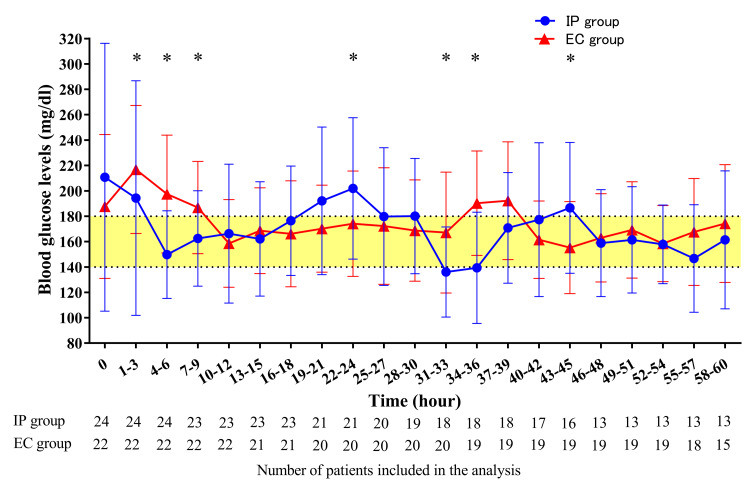
Introduction Glycemic control following pancreatectomy presents challenges, especially in patients with diabetes due to a lack of endogenous insulin, however, optimal management remains unclear. This study evaluated the efficacy and safety of a continuous intravenous insulin infusion protocol employed at our institution, in comparison with conventional glycemic control in patients with pancreatectomy. Materials and methods Sixty-one patients with preoperative glycosylated hemoglobin (HbA1c) of 6.5% or higher, on diabetes medications, or who underwent total pancreatectomy were included. Patients were categorized into three groups: insulin protocol (IP group, n = 24), subcutaneous injection (SI group, n = 15), and continuous intravenous insulin infusion based on the empirical control (EC group, n = 22). The primary outcomes were average blood glucose levels and the proportion of achievement within the target blood glucose range (140-180 mg/dl). Additionally, factors associated with the insulin dose in the IP group were analyzed. Results At predefined time points, the IP group achieved a significantly higher proportion of the target blood glucose range than the SI group (46.2% vs. 31.6%, p = 0.01), with no significant difference in average blood glucose levels (164.1 ± 41.8 vs. 169.1 ± 51.0 mg/dl, p = 0.50). During the 60-hour period following the initiation of frequent blood glucose measurements, the IP group demonstrated significantly reduced average blood glucose levels than the EC group (170.1 ± 56.0 vs. 175.5 ± 43.5 mg/dl, p <0.001), despite significantly longer measurement intervals (1.5 ± 0.7 vs. 1.2 ± 0.7 hours, p <0.001). However, there was no significant difference in the proportion of the target blood glucose range between the IP and EC groups (37.2% vs. 41.0%, p = 0.11). Aspartate transaminase and alanine transferase levels on postoperative day one were positively correlated with the average insulin dose in the IP group (both R = 0.45, p = 0.03). Conclusions This IP helped stabilize blood glucose levels compared to subcutaneous injections and improved glycemic control more effectively than empirically administered continuous intravenous insulin infusion. Postoperative elevations in liver enzymes may serve as predictors of increased insulin requirements.
Keywords: diabetes; glycemic control; insulin protocol; intravenous insulin infusion; pancreatectomy; postoperative hyperglycemia.
Copyright © 2025, Sasaki et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Continuous Subcutaneous Insulin Infusion (CSII) Pumps for Type 1 and Type 2 Adult Diabetic Populations: An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2009;9(20):1-58. Epub 2009 Oct 1. Ont Health Technol Assess Ser. 2009. PMID: 23074525 Free PMC article.
-
Diabetes management in patients undergoing total pancreatectomy: A single center cohort study.Front Endocrinol (Lausanne). 2023 Feb 13;14:1097139. doi: 10.3389/fendo.2023.1097139. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 36860372 Free PMC article.
-
The effectiveness of continuous subcutaneous insulin pumps with continuous glucose monitoring in outpatient adolescents with type 1 diabetes: A systematic review.JBI Libr Syst Rev. 2012;10(42 Suppl):1-10. doi: 10.11124/jbisrir-2012-170. JBI Libr Syst Rev. 2012. PMID: 27820140
-
Rapid-Acting Insulin Analogues Versus Regular Human Insulin: A Meta-Analysis of Effects on Glycemic Control in Patients with Diabetes.Diabetes Ther. 2020 Mar;11(3):573-584. doi: 10.1007/s13300-019-00732-w. Epub 2019 Dec 23. Diabetes Ther. 2020. PMID: 31873857 Free PMC article. Review.
-
Addressing hyperglycemia from hospital admission to discharge.Curr Med Res Opin. 2010 Mar;26(3):589-98. doi: 10.1185/03007990903566822. Curr Med Res Opin. 2010. PMID: 20078323 Review.
References
-
- Stress hyperglycemia during surgery and anesthesia: pathogenesis and clinical implications. Palermo NE, Gianchandani RY, McDonnell ME, Alexanian SM. Curr Diab Rep. 2016;16:33. - PubMed
-
- Postoperative hyperglycemia and adverse outcomes in patients undergoing colorectal surgery: results from the Michigan surgical quality collaborative database. Mohan S, Kaoutzanis C, Welch KB, et al. Int J Colorectal Dis. 2015;30:1515–1523. - PubMed
-
- Persistent postoperative hyperglycemia as a risk factor for operative treatment of deep wound infection after spine surgery. Pennington Z, Lubelski D, Westbroek EM, Ahmed AK, Passias PG, Sciubba DM. Neurosurgery. 2020;87:211–219. - PubMed
LinkOut - more resources
Full Text Sources