

Comparing hemodialysis and hemodiafiltration performance with and without hemoadsorption
- PMID: 40400788
- PMCID: PMC12093098
- DOI: 10.1093/ckj/sfaf146
Comparing hemodialysis and hemodiafiltration performance with and without hemoadsorption
Abstract
Background: New cartridges have been developed using the latest resins for hemoadsorption (HA). When used alongside dialyzers, these cartridges may enhance the removal of certain uremic toxins achieved with classical diffusion and convection. This study aimed to assess the elimination of a wide range of molecular weight solutes, including protein-bound uremic toxins, in hemodialysis (HD) and postdilution hemodiafiltration (HDF) treatments.
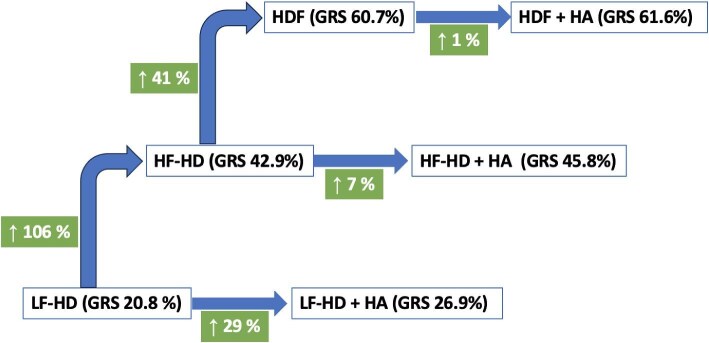
Methods: A prospective study was conducted involving 20 patients who underwent six dialysis sessions with routine treatment parameters maintenance, while only the dialysis modality was modified. The modalities included low-flux HD (LFHD), LFHD-HA, high-flux HD (HFHD), HFHD-HA, HDF and HDF-HA.
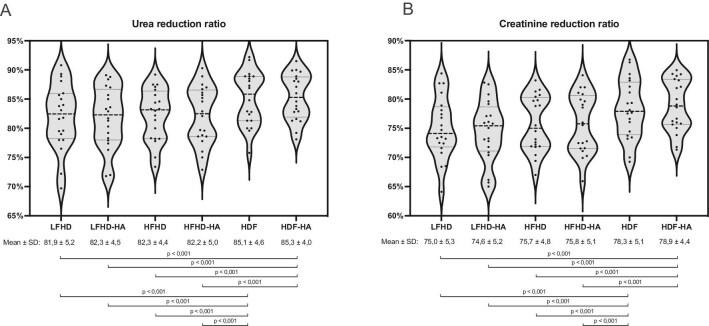
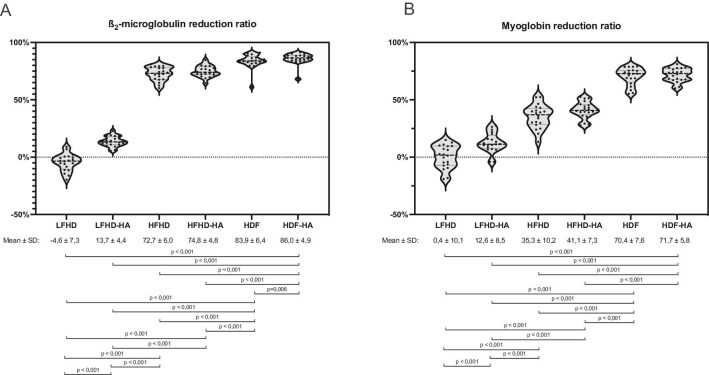
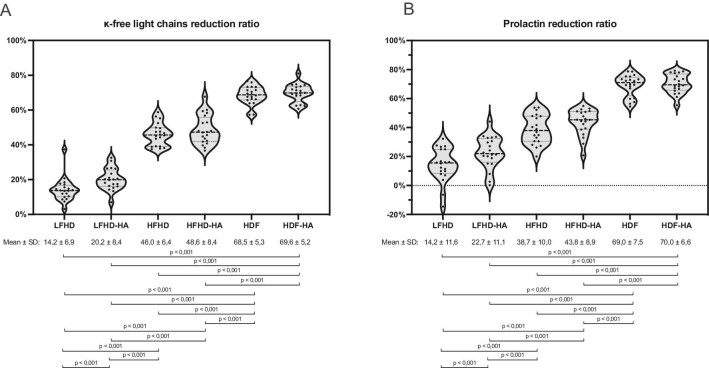
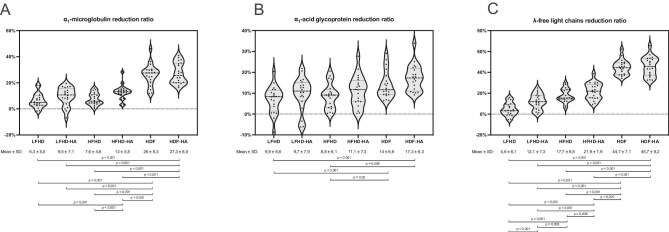
Results: Urea and creatinine reduction ratios (RR) were higher in HDF treatments (with or without HA) versus LFHD and HFHD treatments. In the same treatment modality, the addition of HA did not modify the small molecules removal. The combination of LFHD-HA showed increased RR of β2-microglobulin, myoglobin, prolactin and lambda-free immunoglobulin light chains (λFLC) compared with HD alone. Similarly, the combination of HFHD-HA showed increased RR of myoglobin, α1-microglobulin and λFLC compared with HFHD alone. However, in terms of HDF, the addition of HA tended to slightly increase RR, but only those of β2-microglobulin were significant. Overall, HDF both with and without HA was clearly superior to LFHD and HFHD treatments. Moreover, regardless of the addition of HA, HFHD was superior to LFHD treatments.
Conclusions: The results confirmed the superiority of postdilution HDF over LFHD and HFHD, as well as HFHD over LFHD. Incorporating adsorption into the standard LFHD diffusion significantly enhanced the removal of uremic toxins, whose clearance is restricted by the dialyzer's pore size. In contrast, incorporating adsorption alongside the typical diffusion and convection resulted in a modest enhancement in HFHD, with similar outcomes for HDF.
Keywords: hemoadsorption; hemodiafiltration; hemodialysis; performance; reduction ratios.
© The Author(s) 2025. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
F.M. has received consultancy fees and lecture fees from Baxter, Fresenius Medical Care, Medtronic, Nipro, Nikkiso, Toray and Vifor. J.J.B. has received lecture fees from Fresenius Medical Care. The other authors declare no conflicts of interest.
Figures



References
LinkOut - more resources
Full Text Sources
Research Materials
