

Computed tomography imaging features in Stanford type-A aortic dissection predict in-hospital rupture
- PMID: 40400960
- PMCID: PMC12090109
- DOI: 10.21037/jtd-24-1702
Computed tomography imaging features in Stanford type-A aortic dissection predict in-hospital rupture
Abstract
Background: Aortic rupture is a leading cause of early mortality in patients with Stanford type A aortic dissection (TAAD). Current risk assessment models lack critical imaging features, which could enhance their accuracy and sensitivity. This study aimed to identify potential imaging-based risk factors for in-hospital aortic rupture in patients with TAAD.
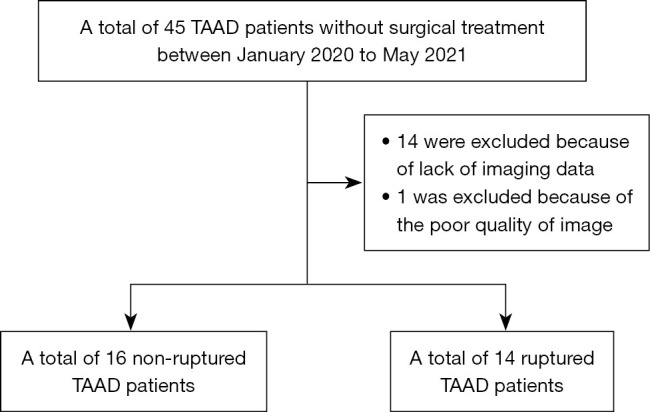
Methods: We conducted a retrospective cross-sectional study of TAAD cases treated medically between January 2020 and May 2021 at Xiamen Cardiovascular Hospital. A total of 45 patients were initially enrolled; however, 14 patients who did not undergo computed tomography angiography (CTA) at Xiamen Cardiovascular Hospital and 1 patient whose quality of image was poor were excluded. We analyzed clinical data, including basic characteristics, clinical presentations, and morphological features derived from CTA and reconstructed images for the remaining 30 patients.
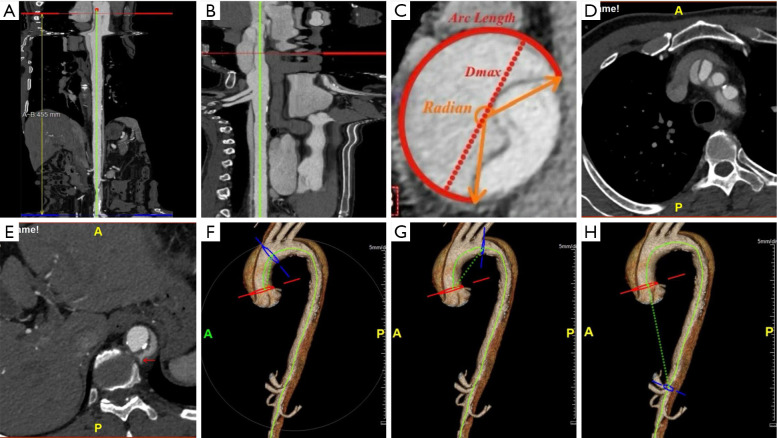
Results: Aortic rupture accounted for 82% (14/17) of in-hospital deaths among conservatively treated patients with TAAD. Patients who experienced rupture demonstrated a significantly higher proportion of dissected false lumen (P=0.04), a longer false lumen arc length (P=0.02), and an increased distance from the sinotubular junction to the origin of the celiac trunk (P=0.02). Single factor logistic regression analysis identified two risk factors: arc length ≥130 mm (odds ratio =5.78; 95% confidence interval: 1.12-29.85; P=0.04) and centerline distance from the sinotubular junction to the origin of the celiac trunk ≥391 mm (odds ratio =11; 95% confidence interval: 2-60.57; P=0.006).
Conclusions: Morphological features observed on computed tomography imaging can serve as valuable predictors for the risk of aortic rupture in patients with TAAD. Incorporating these features into predictive models could improve risk stratification, allowing for earlier surgical intervention in patients at the highest risk of rupture.
Keywords: Stanford type A aortic dissection (TAAD); aortic rupture; imaging features; risk factor.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-1702/coif). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources