

The role of postoperative radiotherapy for invasive thymic epithelial tumors: a single-center experience
- PMID: 40400973
- PMCID: PMC12090111
- DOI: 10.21037/jtd-24-1805
The role of postoperative radiotherapy for invasive thymic epithelial tumors: a single-center experience
Abstract
Background: Surgery is the primary treatment modality for thymic epithelial tumors (TETs). However, the efficacy of postoperative radiotherapy (PORT) in the management of thymoma remains a topic of debate. This study aimed to evaluate the role of PORT in improving clinical outcomes for patients with thymoma.
Methods: We retrospectively analyzed data from patients who underwent surgery for TETs at the Cardiovascular Thoracic Surgery Department, Tianjin Medical University General Hospital from October 2001 to July 2021. Patients classified as Masaoka-Koga stage II to IVA were included in the study. The impact of PORT on relapse-free survival (RFS) and overall survival (OS) was assessed using the Kaplan-Meier method and Cox proportional hazards regression analysis.
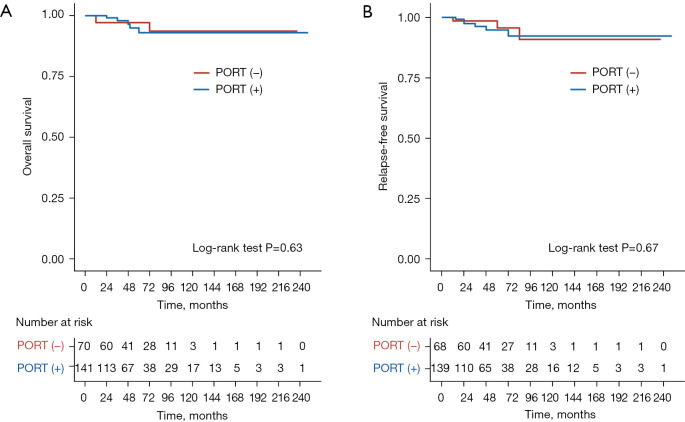
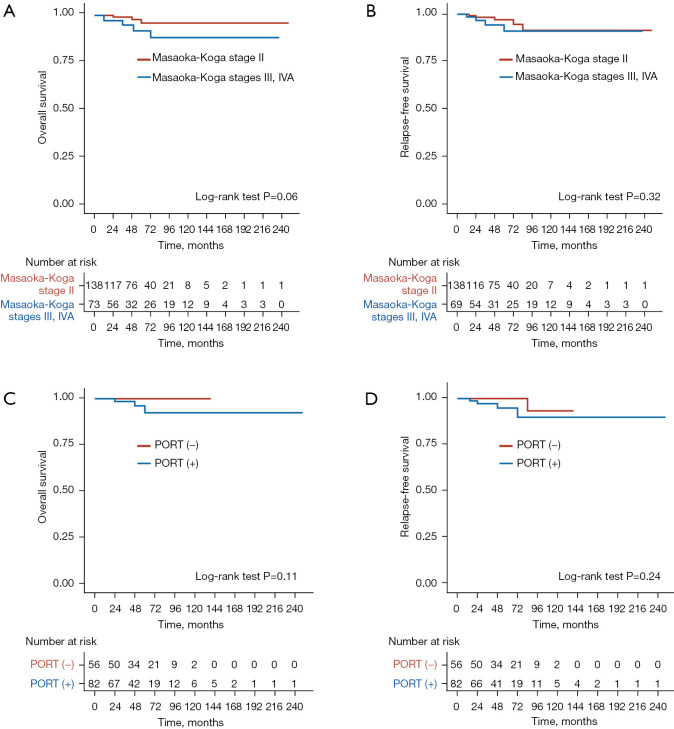
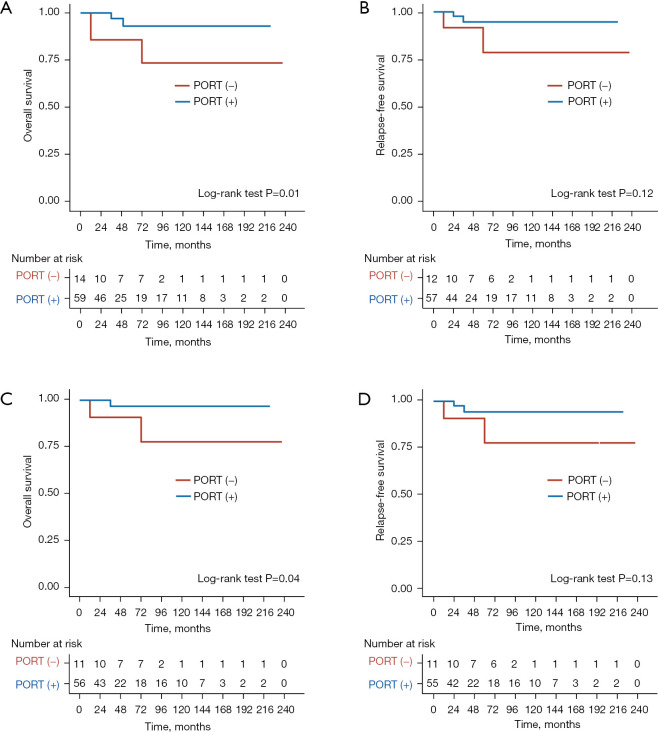
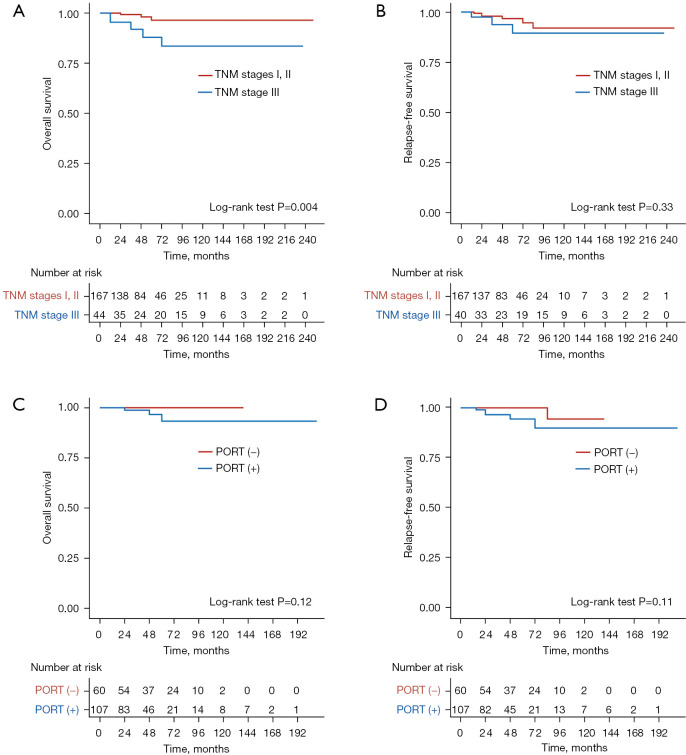
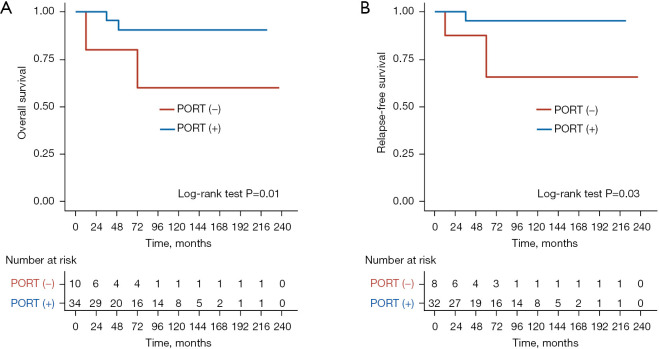
Results: A total of 211 thymoma patients were included in this study, among whom 141 cases (66.8%) underwent PORT. Overall, PORT was not associated with a significant improvement in OS or RFS in the entire cohort. However, in patients with locally advanced disease, PORT for Masaoka-Koga stage III-IVA thymoma was significantly associated with improved OS (P=0.01), although it did not result in a significant improvement in RFS (P=0.12). Subgroup analyses revealed that PORT significantly improved OS (P=0.042) in patients with Masaoka-Koga stage III thymoma. Furthermore, among patients with tumor-node-metastasis (TNM) stage III thymoma [according to the Union for the International Cancer Control (UICC) TNM Classification, 8th Edition], the PORT group exhibited significantly better RFS (P=0.03) and OS (P=0.01). Cox regression analysis demonstrated that TNM stage was the only statistically significant factor influencing OS in univariate analysis among patients with aggressive thymoma [TNM stage I-II vs. TNM stage III, hazard ratio (HR): 5.669, 95% confidence interval (CI): 1.347-23.852, P=0.02]. In addition, PORT was the only statistically significant factor influencing OS in univariate analysis for patients with TNM stage III thymoma (PORT vs. non-PORT, HR: 13.646, 95% CI: 1.522-122.356, P=0.02).
Conclusions: PORT plays a significant role in the management of thymoma patients. For patients with Masaoka-Koga stage II thymoma, the potential benefits of PORT require further investigation. In patients with Masaoka-Koga stage III-IVA thymoma, PORT is associated with improved OS but does not appear to prevent disease recurrence. Additionally, among TNM stage III patients, the PORT group demonstrated significantly better RFS and OS. TNM stage is a potentially independent prognostic factor for survival in patients with aggressive thymoma, while PORT represents a critical prognostic factor for survival in patients with TNM stage III thymoma.
Keywords: Postoperative radiotherapy (PORT); thymoma; tumor-node-metastasis stage (TNM stage).
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-1805/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Postoperative radiotherapy is effective for thymic carcinoma but not for thymoma in stage II and III thymic epithelial tumors: the Japanese Association for Research on the Thymus Database Study.Cancer. 2015 Apr 1;121(7):1008-16. doi: 10.1002/cncr.29166. Epub 2015 Jan 6. Cancer. 2015. PMID: 25565590
-
The Studies of Prognostic Factors and the Genetic Polymorphism of Methylenetetrahydrofolate Reductase C667T in Thymic Epithelial Tumors.Front Oncol. 2022 Jun 6;12:847957. doi: 10.3389/fonc.2022.847957. eCollection 2022. Front Oncol. 2022. PMID: 35734597 Free PMC article.
-
The Impact of Postoperative Radiotherapy for Thymoma and Thymic Carcinoma.J Thorac Oncol. 2017 Apr;12(4):734-744. doi: 10.1016/j.jtho.2017.01.002. Epub 2017 Jan 25. J Thorac Oncol. 2017. PMID: 28126540
-
The value of postoperative radiotherapy in thymoma patients with myasthenia gravis.Radiother Oncol. 2023 Jun;183:109644. doi: 10.1016/j.radonc.2023.109644. Epub 2023 Mar 27. Radiother Oncol. 2023. PMID: 36990391 Review.
-
Postoperative Radiotherapy for Completely Resected Masaoka/Masaoka-Koga Stage II/III Thymoma Improves Overall Survival: An Updated Meta-Analysis of 4746 Patients.J Thorac Oncol. 2021 Apr;16(4):677-685. doi: 10.1016/j.jtho.2020.12.023. Epub 2021 Jan 27. J Thorac Oncol. 2021. PMID: 33515812
References
LinkOut - more resources
Full Text Sources