

Tumor peripheral bronchial signature predicts spread through air spaces in resected invasive mucinous adenocarcinoma of the lung
- PMID: 40400986
- PMCID: PMC12090135
- DOI: 10.21037/jtd-2024-2036
Tumor peripheral bronchial signature predicts spread through air spaces in resected invasive mucinous adenocarcinoma of the lung
Abstract
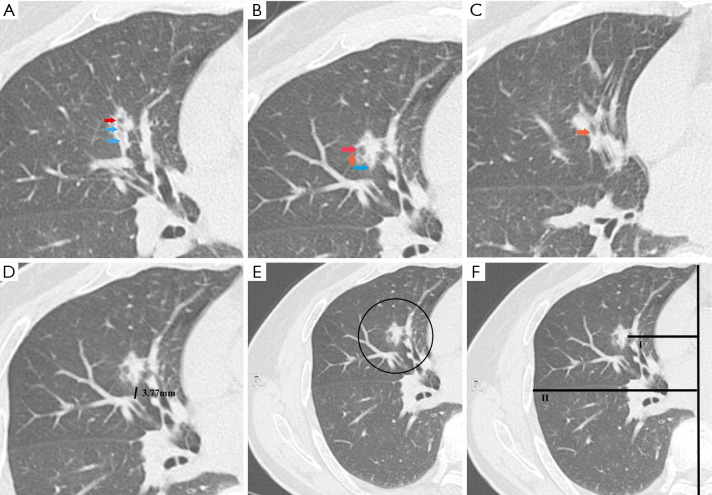
Background: While a higher incidence of spread through air spaces (STAS) has been reported in invasive mucinous adenocarcinoma (IMA) of lung, most studies have only focused on non-mucinous adenocarcinoma (ADC). In this study, tumor peripheral bronchial signature (TPBS) was defined as indicators to describe bronchial morphological changes and bronchial distribution characteristics around the tumor in the preoperative computed tomography (CT) images. The value of TPBS was examined in predicting STAS in patients with resected IMA.
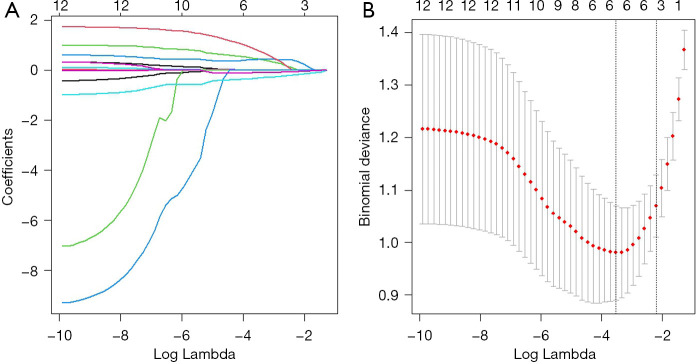
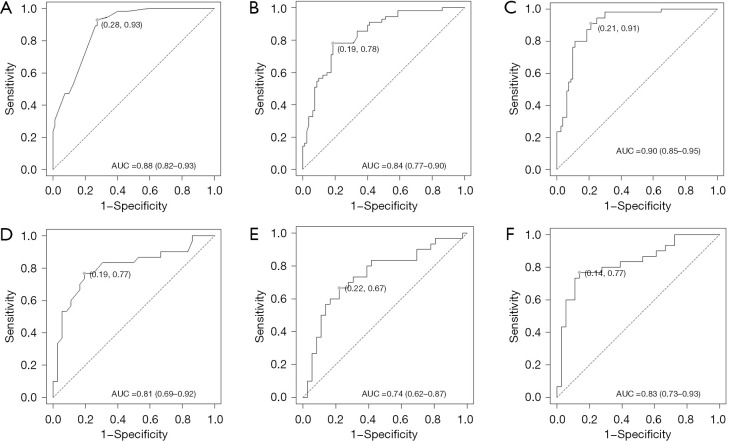
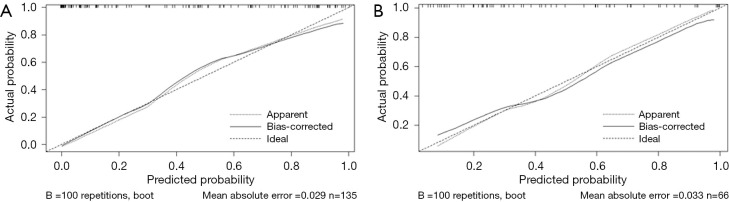
Methods: In the training cohort, the least absolute shrinkage and selection operator (LASSO) method was adopted to identify TPBS that was most strongly associated with STAS, and a formula of TPBS score was constructed. Subsequently, variations in clinical characteristics, radiological features, and TPBS scores were analyzed and compared using both univariate and multivariate statistical methods. Receiver operation characteristic (ROC) curve, decision curve, and calibration curve were employed to evaluate the model's efficacy.
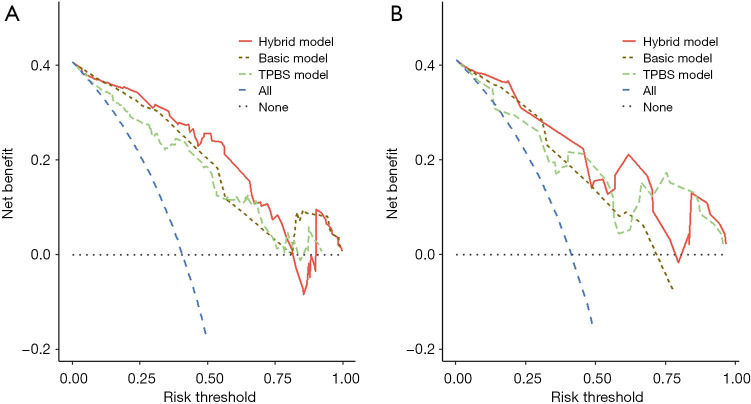
Results: The best predictors included clinical T classification, spiculated margin, combined pneumonia, consolidation-tumor ratio (CTR) and TPBS score. In addition, three different STAS prediction models were developed and the corresponding area under the curve (AUC) values were 0.904, 0.877 and 0.838, respectively. Calibration curve illustrated that the predicted probability value generated by the hybrid model aligned well with the actual STAS status. Moreover, decision curve analysis (DCA) suggested that the hybrid model provided superior clinical utility and application value compared to both the basic model and the TPBS model.
Conclusions: TPBS score was identified as an independent predicting factor for STAS status. The nomogram, utilizing radiological features and TPBS score, demonstrated a high level of diagnostic accuracy and efficiency in predicting the status of STAS.
Keywords: Spread through air spaces (STAS); invasive mucinous adenocarcinoma (IMA); prediction; tumor peripheral bronchial signature (TPBS).
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2024-2036/coif). The authors have no conflicts of interest to declare.
Figures


Similar articles
-
Nomogram based on clinical characteristics and radiological features for the preoperative prediction of spread through air spaces in patients with clinical stage IA non-small cell lung cancer: a multicenter study.Diagn Interv Radiol. 2023 Nov 7;29(6):771-785. doi: 10.4274/dir.2023.232404. Epub 2023 Sep 19. Diagn Interv Radiol. 2023. PMID: 37724737 Free PMC article. Clinical Trial.
-
Spread through air spaces (STAS) in invasive mucinous adenocarcinoma of the lung: Incidence, prognostic impact, and prediction based on clinicoradiologic factors.Thorac Cancer. 2020 Nov;11(11):3145-3154. doi: 10.1111/1759-7714.13632. Epub 2020 Sep 25. Thorac Cancer. 2020. PMID: 32975379 Free PMC article.
-
Preoperative CT radiomic model combined with clinical and CT imaging features to predict the spread through air spaces in T1 invasive lung adenocarcinoma.Am J Transl Res. 2024 Oct 15;16(10):6106-6118. doi: 10.62347/UJYU8551. eCollection 2024. Am J Transl Res. 2024. PMID: 39544799 Free PMC article.
-
Prognostic factors for invasive mucinous adenocarcinoma of the lung: systematic review and meta-analysis.World J Surg Oncol. 2024 Feb 2;22(1):41. doi: 10.1186/s12957-024-03326-4. World J Surg Oncol. 2024. PMID: 38303008 Free PMC article.
-
A narrative review of preoperative CT for predicting spread through air spaces of lung cancer.Transl Lung Cancer Res. 2025 Apr 30;14(4):1471-1481. doi: 10.21037/tlcr-24-952. Epub 2025 Apr 27. Transl Lung Cancer Res. 2025. PMID: 40386727 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources