

Epicardial ablation in high-risk Brugada syndrome to prevent ventricular fibrillation: results from a randomized clinical trial
- PMID: 40401314
- PMCID: PMC12096002
- DOI: 10.1093/europace/euaf097
Epicardial ablation in high-risk Brugada syndrome to prevent ventricular fibrillation: results from a randomized clinical trial
Abstract
Aims: Epicardial ablation for Brugada syndrome (BrS) has shown promise in reducing ventricular fibrillation (VF), but its role remains controversial due to the lack of randomized trials. This study evaluates the efficacy of catheter ablation in high-risk BrS patients.
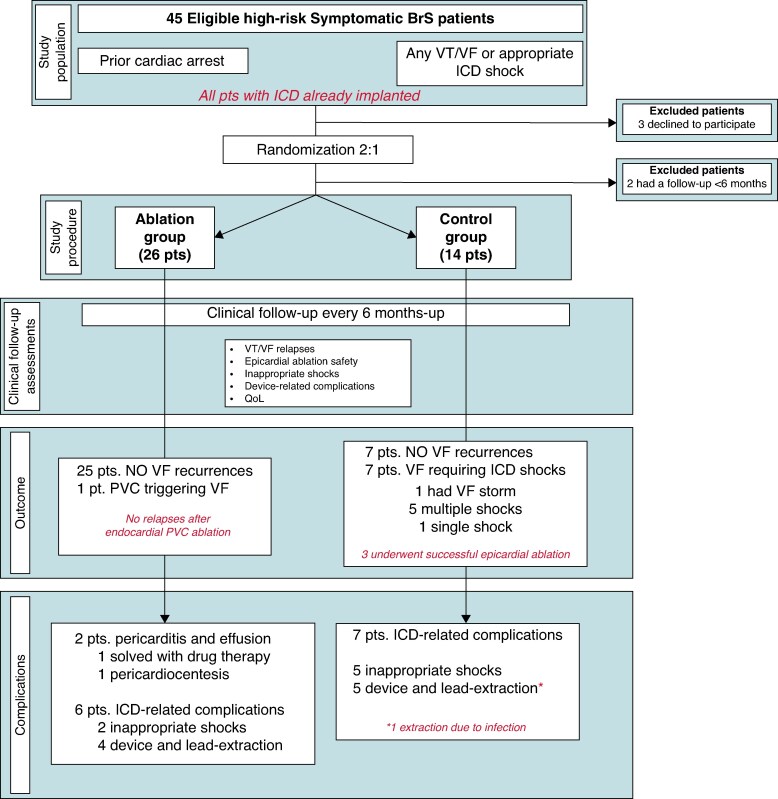
Methods and results: This prospective, single-centre, randomized (2:1) study enrolled BrS patients with cardiac arrest (CA) or appropriate ICD therapies. All patients had an ICD and were randomized to undergo epicardial ablation (ablation group) or no ablation (control group). Enrolment began in September 2017 and prematurely terminated in February 2024. The primary endpoint was freedom from VF recurrences. Secondary endpoints included procedure safety, ICD-related complications, and quality-of-life assessment. Forty patients (83% male, mean age 43.7 ± 12.1) were randomized: 26 in the ablation group and 14 in the control group. Thirty-six patients received appropriate ICD therapies before enrolment: 24 (92%) in the ablation group and 12 (86%) in the control group. One patient in the ablation group experienced a post-procedural pericardial effusion requiring pericardiocentesis. Thirteen patients (33%) had major ICD-related complications. After a mean follow-up of 4.0 ± 1.7 years, freedom from VF recurrence was 96% (25/26) in the ablation group and 50% (7/14) in the control group (P < 0.001). No unexplained or arrhythmic deaths occurred during follow-up.
Conclusion: Epicardial catheter ablation was associated with a reduction in VF recurrence compared with ICD therapy alone. These findings support the use of epicardial ablation in high-risk BrS patients.
Clinicaltrials.gov: ID NCT03294278.
Keywords: Arrhythmogenic substrate; Brugada syndrome; Cardiac arrest; Epicardium; ICD; Ventricular fibrillation.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: The authors have nothing to disclose.
Figures





Comment in
-
Accumulating evidence for epicardial ablation in malignant forms of Brugada syndrome: summary of two randomized clinical trials.Europace. 2025 Jun 3;27(6):euaf116. doi: 10.1093/europace/euaf116. Europace. 2025. PMID: 40590688 Free PMC article. No abstract available.
References
-
- Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;43:3997–4126. - PubMed
-
- Probst V, Plassard-Kerdoncuf D, Mansourati J, Mabo P, Sacher F, Fruchet C et al. The psychological impact of implantable cardioverter defibrillator implantation on Brugada syndrome patients. Europace 2011;13:1034–9. - PubMed
-
- Andorin A, Gourraud JB, Mansourati J, Fouchard S, le Marec H, Maury P et al. The QUIDAM study: hydroquinidine therapy for the management of Brugada syndrome patients at high arrhythmic risk. Heart Rhythm 2017;14:1147–54. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
