

Neurological Evaluation of Severe Congenital Kyphosis With Compressive Myelopathy in 39 Patients With a Minimum 1-Year Follow-Up
- PMID: 40401546
- PMCID: PMC12214409
- DOI: 10.1111/os.70070
Neurological Evaluation of Severe Congenital Kyphosis With Compressive Myelopathy in 39 Patients With a Minimum 1-Year Follow-Up
Abstract
Objective: Congenital angular kyphosis with compressive myelopathy is a rare yet underreported neurologic emergency for spine surgeons. The study aimed to report the neurological outcomes of 39 patients with compressive myelopathy in congenital kyphosis (CK) and provide magnetic resonance imaging (MRI) features in these patients, identifying the potential prognostic factors.
Methods: This is a retrospective cohort study. From January 2010 to December 2022, 39 patients were diagnosed with severe congenital angular kyphosis with compressive myelopathy and received surgical correction. The American Spinal Injury Association (ASIA) Impairment Scale grades at admission and final follow-up were recorded to measure neurological outcomes. A series of qualitative and quantitative parameters were evaluated on preoperative MRI by observers who were blinded to the clinical outcomes. According to the final status of neurological recovery, patients were divided into two groups and compared: Group E (patients with ASIA E) and Group N (patients with ASIA A, B, C, and D).
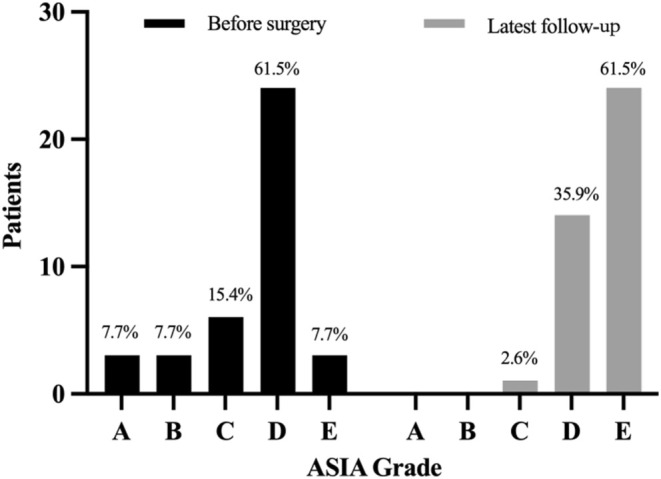
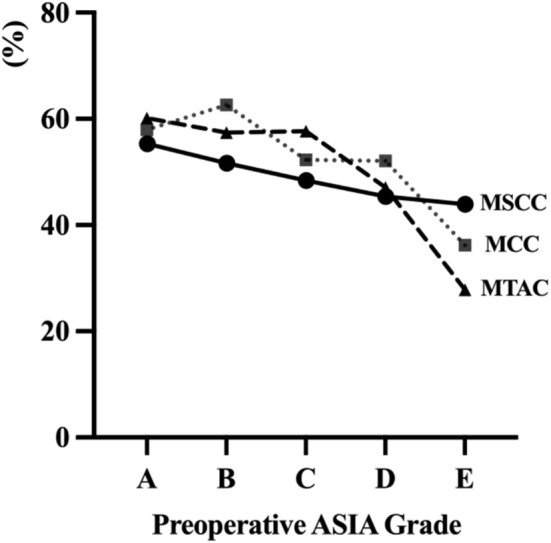
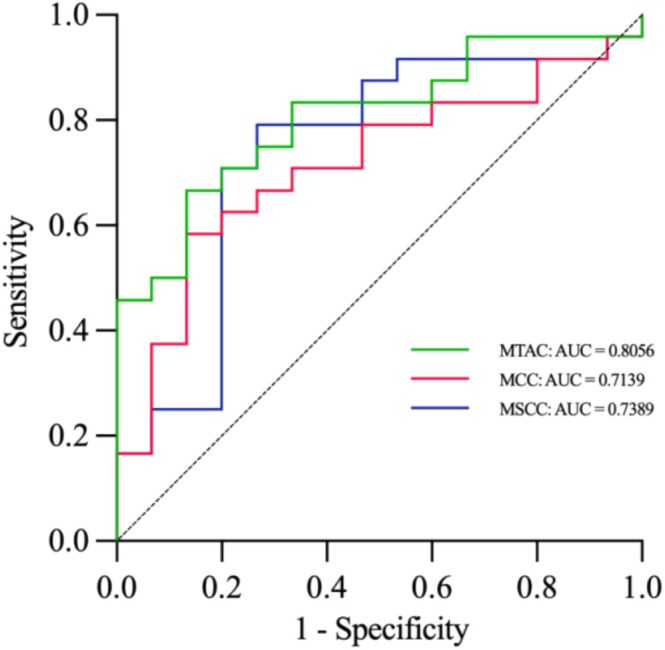
Results: At the final follow-up, 79.5% of patients (31 cases) had improved neurological function and myelopathy symptoms. The average Cobb angle of kyphosis decreased from 78.4° to 20.1° after correction surgery. The duration of myelopathy in Group N was significantly longer than that in Group E (p = 0.038). T1-weighted imaging (T1WI) signal hypointensity was presented in 35.9% (14/39) of patients, and T2-weighted imaging (T2WI) signal hyperintensity was 69.2% (27/39). On average, these patients had a maximum canal compromise (MCC) of 52.2%, maximum spinal cord compression (MSCC) of 47.0%, and maximum transverse area compression (MTAC) of 49.1%. Compared to Group E, Group N showed greater MCC (p = 0.023), MSCC (p = 0.008), and MTAC (p < 0.001) at baseline, and was more likely to present T1WI hypointensity and T2WI hyperintensity. The cut-off values of MTAC, MCC, and MSCC for fully neurological recovery were 47.1%, 46.7%, and 52.6%, respectively.
Conclusion: MRI indicators of poor prognosis in CK patients with compressive myelopathy included the presence of T1WI hypointensity, T2WI hyperintensity, and greater MCC, MSCC, and MTAC. It was suggested that early surgical intervention is critical to prevent irreversible cord injury, particularly in patients with MTAC > 47.1%.
Keywords: compressive myelopathy; congenital angular kyphosis; magnetic resonance imaging; neurological dysfunction.
© 2025 The Author(s). Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Late-Onset Spinal Cord Dysfunction in Rigid Posttraumatic Thoracolumbar Kyphosis: Radiographic Analysis of Neurological Compromise.Orthop Surg. 2025 Jul;17(7):2048-2056. doi: 10.1111/os.70075. Epub 2025 May 23. Orthop Surg. 2025. PMID: 40405744 Free PMC article.
-
Effect of diabetes mellitus on spinal cord high signal relief after anterior cervical spine surgery in patients with cervical spondylotic myelopathy.BMC Surg. 2025 Jul 3;25(1):268. doi: 10.1186/s12893-025-03025-1. BMC Surg. 2025. PMID: 40611185 Free PMC article.
-
Assessment of spinal cord compression by magnetic resonance imaging--can it predict surgical outcomes in degenerative compressive myelopathy? A systematic review.Spine (Phila Pa 1976). 2013 Jul 15;38(16):1409-21. doi: 10.1097/BRS.0b013e31829609a0. Spine (Phila Pa 1976). 2013. PMID: 23591658
-
Should dry spinal tuberculosis be managed differently than wet spinal tuberculosis?Spine J. 2025 Jul;25(7):1455-1465. doi: 10.1016/j.spinee.2025.01.002. Epub 2025 Jan 16. Spine J. 2025. PMID: 39826703
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
References
-
- McMaster M. J. and Singh H., “Natural History of Congenital Kyphosis and Kyphoscoliosis. A Study of One Hundred and Twelve Patients,” Journal of Bone and Joint Surgery. American Volume 81 (1999): 1367–1383. - PubMed
-
- McMaster M. J., “Spinal Growth and Congenital Deformity of the Spine,” Spine 31 (2006): 2284–2287. - PubMed
-
- He Z., Liu Y., Xue F., Xiao H., Yuan W., and Chen D., “Surgical Management of Congenital Cervical Kyphosis,” Orthopedics 35 (2012): e1396–e1401. - PubMed
-
- Winter R. B., Moe J. H., and Wang J. F., “Congenital Kyphosis. Its Natural History and Treatment as Observed in a Study of One Hundred and Thirty Patients,” Journal of Bone and Joint Surgery. American Volume 55 (1973): 223–256. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
