

Fasting Before Cardiac Catheterization: Still Necessary? A Systematic Review and Meta-Analysis of Randomized Clinical Trials
- PMID: 40401623
- PMCID: PMC12229180
- DOI: 10.1161/JAHA.124.040445
Fasting Before Cardiac Catheterization: Still Necessary? A Systematic Review and Meta-Analysis of Randomized Clinical Trials
Abstract
Background: Fasting before elective or nonurgent coronary angiography is commonly recommended to reduce the risk of adverse events, such as aspiration pneumonia. This systematic review and meta-analysis aimed to evaluate the impact of fasting versus nonfasting protocols on patient outcomes and satisfaction.
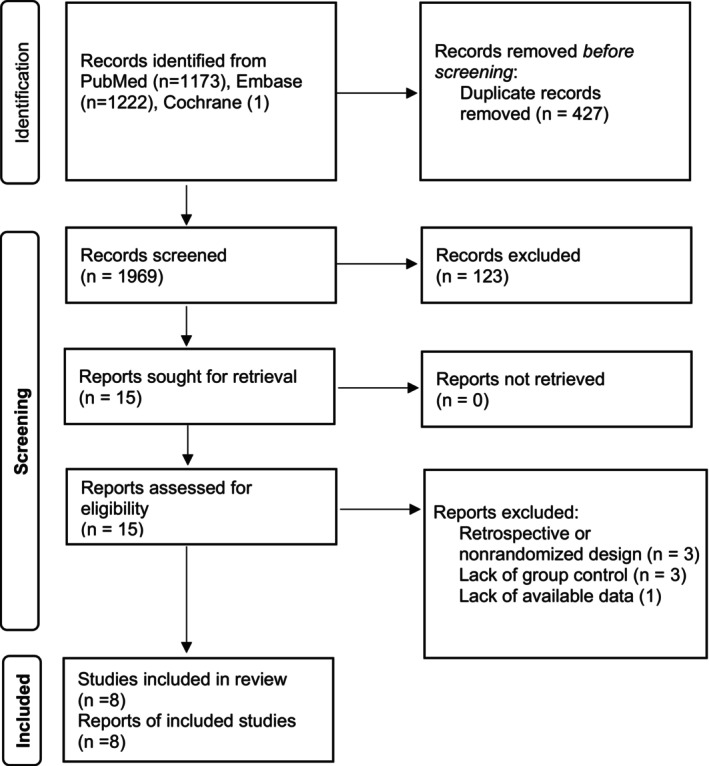
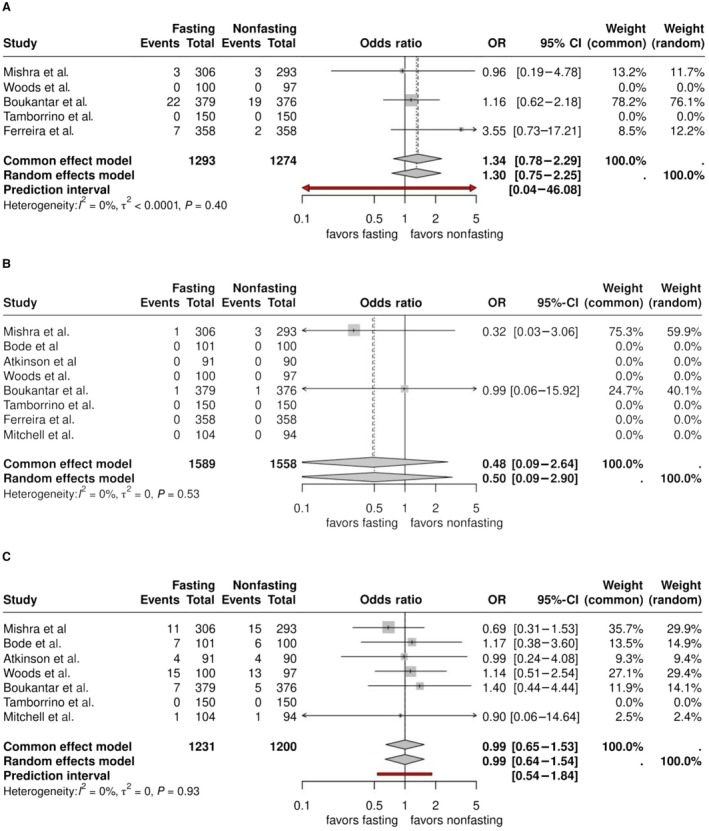
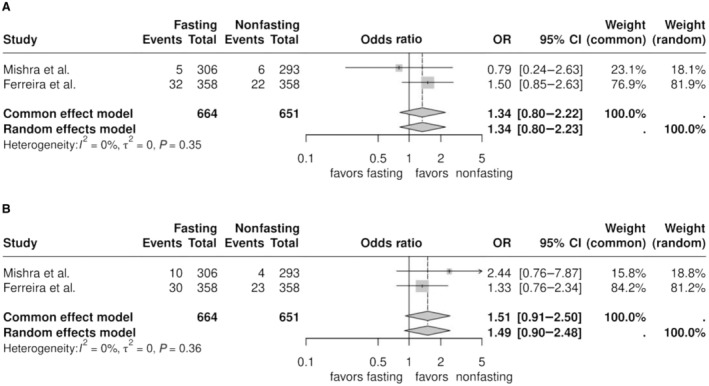
Methods: We systematically searched PubMed, Embase, and Cochrane Library databases for randomized clinical trials comparing fasting and nonfasting states before cardiac catheterization. The primary outcome was a composite of adverse events including pneumonia, hypoglycemia, and nausea/vomiting. Secondary outcomes included individual adverse events and patient satisfaction. For each binary outcome we estimated crude event probabilities for each treatment arm. Next, we pooled study-specific results in meta-analyses using odds ratio (OR) and risk difference as effect measures for binary outcomes and standardized mean difference for satisfaction.
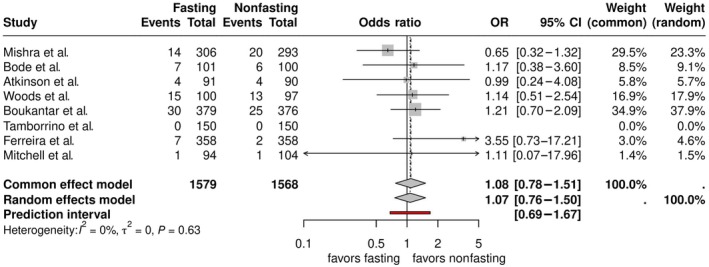
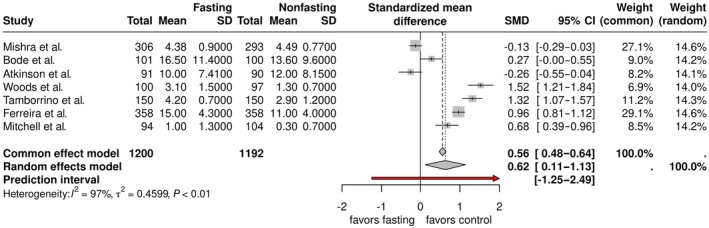
Results: We identified 8 randomized clinical trials, including a total of 3147 patients. Our meta-analysis showed no evidence of a difference in the incidence of composite adverse events between fasting and nonfasting groups in ORs (OR, 1.08, [95% CI, 0.78-1.51], where OR<1 favors fasting). The crude event probabilities were 4.9% and 4.4% for fasting and nonfasting groups respectively, with an estimated risk difference =0.4% (-1.1% to 1.8%), where risk difference <0 favors fasting. Patient satisfaction was found higher in nonfasting protocols, standardized mean difference 0.62 (0.11-1.13).
Conclusion: Our meta-analysis found no evidence that fasting before elective coronary angiography reduces adverse events. However, we found evidence that fasting reduces patient satisfaction. These findings question the necessity of fasting protocols in this context.
Registration: URL: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024595465; Unique identifier: CRD42024595465.
Keywords: cardiac catheterization; fasting; percutaneous coronary intervention.
Conflict of interest statement
None.
Figures
References
-
- Virani SS et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA guideline for the Management of Patients with Chronic Coronary Disease: a report of the American Heart Association/American College of Cardiology Joint Committee on clinical practice guidelines. Circulation. 2023;148:e9–e119. doi: 10.1161/CIR.0000000000001183 - DOI - PubMed
-
- Gulati M et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of CHEST pain: executive summary: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2021;144:e368–e454. doi: 10.1161/CIR.0000000000001047 - DOI - PubMed
-
- Naidu SS et al. SCAI expert consensus update on best practices in the cardiac catheterization laboratory: this statement was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), and the Heart Rhythm Society (HRS) in April 2021. Catheter Cardiovasc Interv. 2021;98:255–276. doi: 10.1002/ccd.29744 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
