

Inter-seizure variability in thalamic recruitment and its implications for precision thalamic neuromodulation
- PMID: 40404918
- PMCID: PMC12098681
- DOI: 10.1038/s43856-025-00920-9
Inter-seizure variability in thalamic recruitment and its implications for precision thalamic neuromodulation
Abstract
Background: Thalamic stimulation is a promising approach to controlling seizures in patients with intractable epilepsy. It does not, however, provide good control for everyone. A big issue is that the role of the thalamus in seizure organization and propagation is unclear. When using responsive stimulation devices, they must detect seizure activity before sending stimulation. So, it's important to know which parts of the thalamus are involved in different seizures.
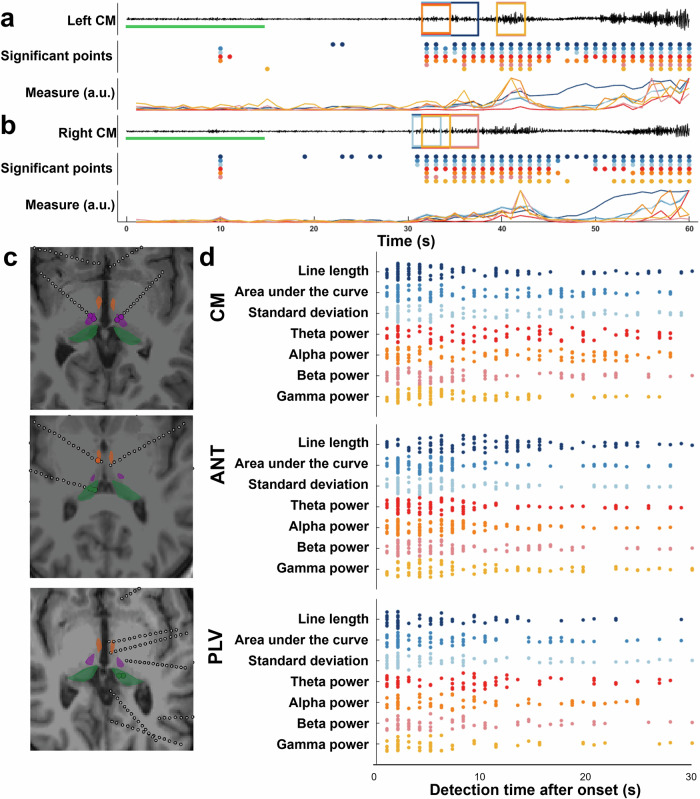
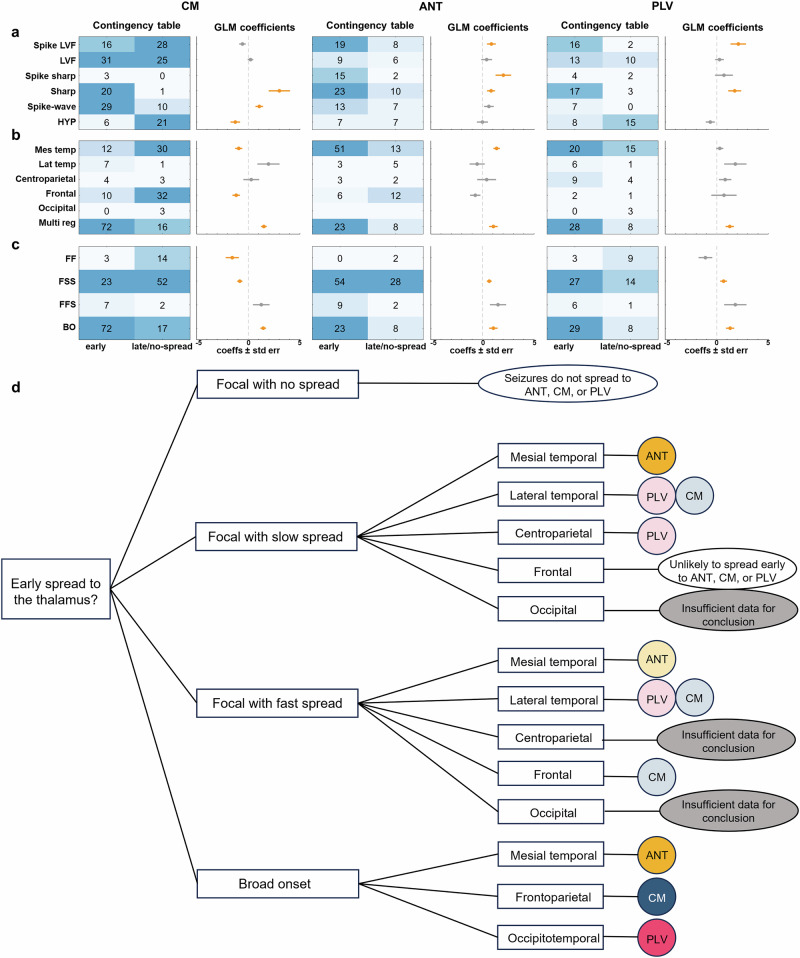
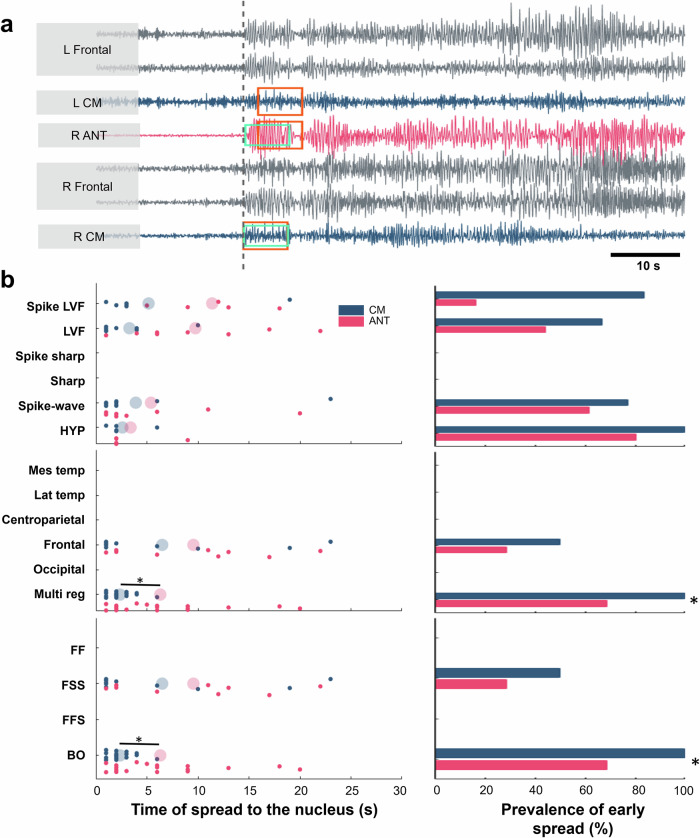
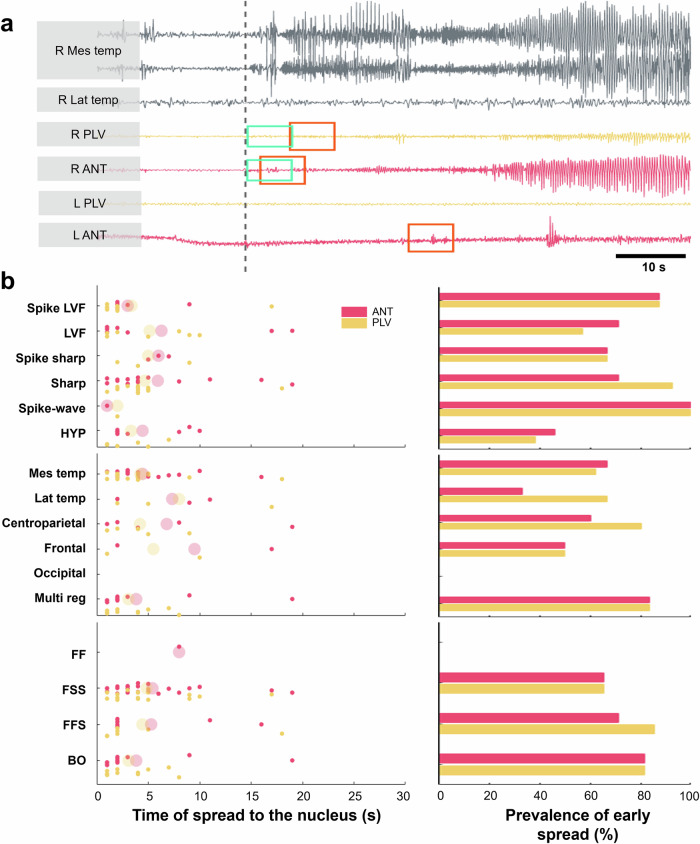
Methods: To better choose thalamic targets for stimulation, we studied how different seizures spread to each stimulation target. Expert reviews and automated tools were used to identify seizure spread recorded from invasive recordings. We categorized seizures based on how they start and spread, and determined whether seizures reached thalamic areas early or late. We used generalized linear models (GLM) to evaluate which seizure properties are predictive of time of spread to the thalamus, testing effect significance using Wald tests.
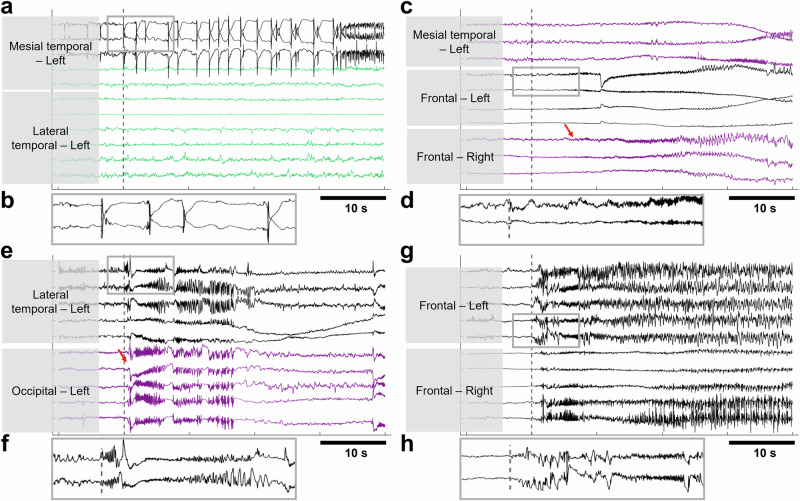
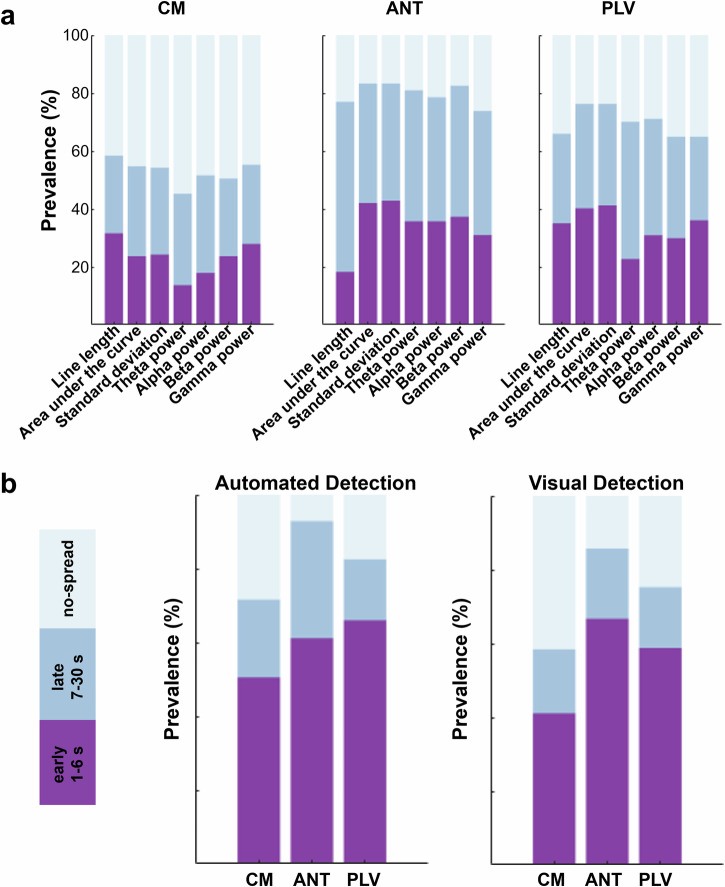
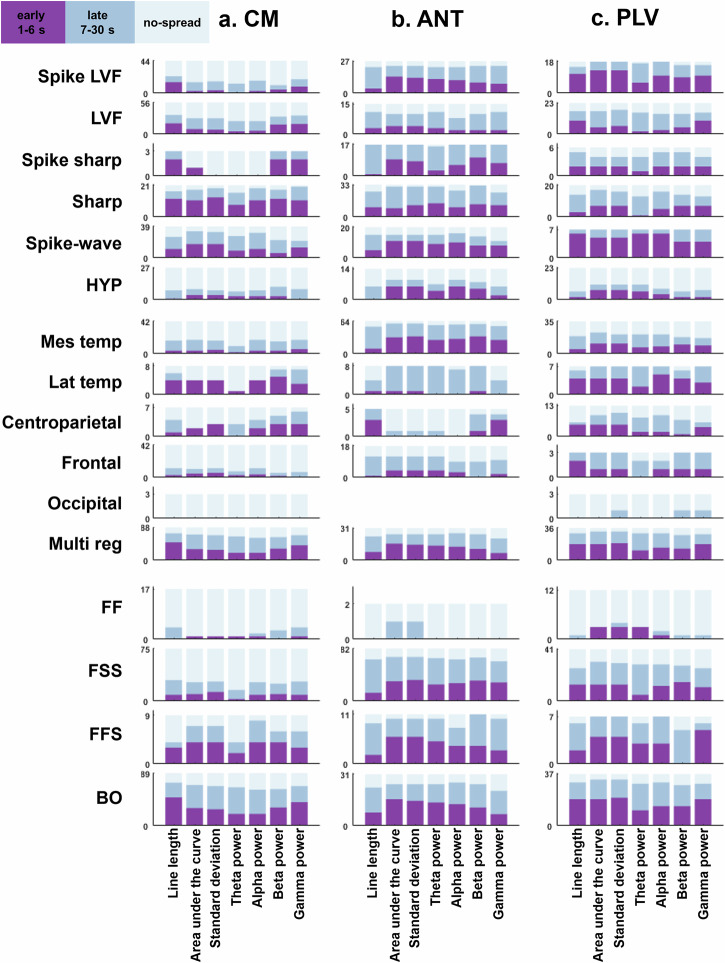
Results: We show that seizures with <2 Hz synchronized-spiking patterns do not spread early to the thalamus, while seizures starting with faster activity (<20 Hz) spread early to all thalamic areas. Most importantly, seizures that begin broadly across the brain quickly recruit the centromedian and pulvinar areas, suggesting these may be better stimulation targets in such cases. Alternatively, seizures that start deep in the temporal lobe tend to involve the anterior part of the thalamus, meaning the centromedian might not be the best choice for those seizures.
Conclusions: Our results suggest that by analyzing electrical activity during seizures, we can better predict which parts of the thalamus are involved. This could lead to more effective stimulation treatments for people with epilepsy.
Plain language summary
Some people with epilepsy don’t get relief from standard treatments and may need brain stimulation to help control their seizures. The thalamus, a deep brain structure, is a promising area for this kind of therapy, but clinicians still don’t know exactly which people with epilepsy will benefit most. In our study, we found that certain brainwave patterns during seizures can help identify which part of the thalamus is most involved. This could lead to more personalized and effective brain stimulation treatments for different types of epilepsy.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures

References
-
- Kwan, P. & Brodie, M. J. Early identification of refractory epilepsy. N. Engl. J. Med.342, 314–319 (2000). - PubMed
-
- Thijs, R. D., Surges, R., O’Brien, T. J. & Sander, J. W. Epilepsy in adults. Lancet393, 689–701 (2019). - PubMed
-
- Ma, B. B. et al. Responsive neurostimulation for regional neocortical epilepsy. Epilepsia61, 96–106 (2020). - PubMed
-
- Ryvlin, P., Rheims, S., Hirsch, L. J., Sokolov, A. & Jehi, L. Neuromodulation in epilepsy: state-of-the-art approved therapies. Lancet Neurol.20, 1038–1047 (2021). - PubMed
Grants and funding
- W81XWH-22-1-0315/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- R01 NS079533/NS/NINDS NIH HHS/United States
- R01 NS062092/NS/NINDS NIH HHS/United States
- R01 NS072023/NS/NINDS NIH HHS/United States
- K24-NS088568/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)
LinkOut - more resources
Full Text Sources