

Postoperative outcomes after minimally invasive esophagectomy: an international cohort study from the Oesophagogastric Anastomosis Audit (OGAA)
- PMID: 40405118
- PMCID: PMC12096545
- DOI: 10.1186/s12893-025-02941-6
Postoperative outcomes after minimally invasive esophagectomy: an international cohort study from the Oesophagogastric Anastomosis Audit (OGAA)
Abstract
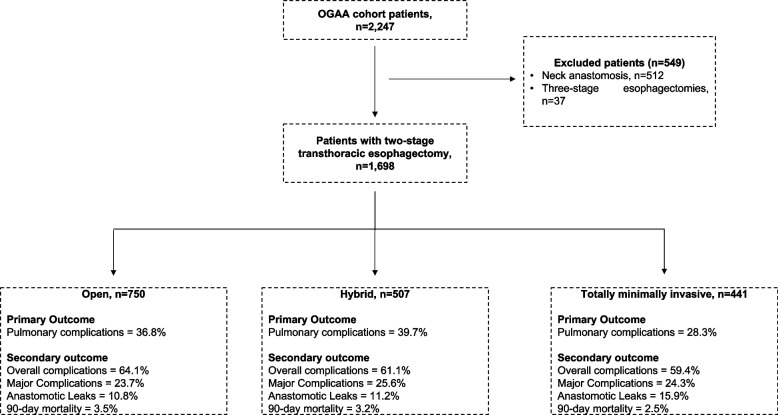
Objective: To compare the postoperative pulmonary complications (PPC) after minimally invasive or open transthoracic esophagectomy for esophageal cancer in an international, multicenter cohort. Ongoing debate exists around the optimal surgical approach for esophageal cancer, with limited data assessing the external validity of randomised trials on outcomes of MIE METHODS: Patients undergoing open (OE, n = 744), hybrid (HE, n = 500), and totally minimally invasive esophagectomy (TMIE, n = 540) for esophageal cancer were identified from the international, prospective Oesophagogastric Anastomosis Audit (OGAA). Multivariable models were used to investigate PPC (primary outcome) as well as overall complications, major complications, anastomotic leak and 90-day mortality (secondary outcomes).
Results: PPC rates were lower after TMIE compared to OE and HE (28% vs 37% vs 39%, p = 0.002), even on adjusted analyses compared to OE (odds ratio (OR): 0.60, CI95%: 0.45-0.78). TMIE was also associated with significantly lower overall complications (OR: 0.68, CI95%: 0.52-0.88) compared to OE, but not for major complications (OR: 0.90, CI95%: 0.67-1.21), anastomotic leak (OR: 1.39, CI95%: 0.96-2.01) and 90-day mortality (OR: 0.49, CI95%: 0.22-1.04). Sensitivity analyses by underlying respiratory disease, neoadjuvant chemoradiotherapy or high-volume centers confirmed above findings.
Conclusion: This study provides real-world data that TMIE was associated with lower 90-day PPC than OE and HE approaches, especially in patients with underlying respiratory disease or receiving neoadjuvant chemoradiotherapy. These warrant a further review into causes and mechanisms in selected patients, and that quality assurance in delivery of TMIE is probably of major importance. The ideal surgical approach remains unclear, and ongoing trials will provide more evidence within a few years that may clarify the optimum approach to locally advanced esophageal cancers.
Keywords: Esophagectomy; Minimally invasive; Outcomes; Pulmonary complications.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval was not applicable for this study, as this was a secondary analysis of cohort study with existing approval. This study was reviewed by the University Hospital Birmingham NHS Trust ethics committee and the need for full ethics review was waived since the study is an observation study of routinely collected data. Informed consent was not needed for all participants in the main study by the ethics committee. This study adhered to the Helsinki declaration. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Shapiro J, van Lanschot JJB, Hulshof M, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, van Laarhoven HWM, Nieuwenhuijzen GAP, Hospers GAP, Bonenkamp JJ, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015;16(9):1090–8. - PubMed
-
- van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, Richel DJ, Nieuwenhuijzen GA, Hospers GA, Bonenkamp JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074–84. - PubMed
-
- Navidi M, Phillips AW, Griffin SM, Duffield KE, Greystoke A, Sumpter K, Sinclair RCF. Cardiopulmonary fitness before and after neoadjuvant chemotherapy in patients with oesophagogastric cancer. Br J Surg. 2018;105(7):900–6. - PubMed
-
- Noordman BJ, Wijnhoven BPL, Lagarde SM, Boonstra JJ, Coene P, Dekker JWT, Doukas M, van der Gaast A, Heisterkamp J, Kouwenhoven EA, et al. Neoadjuvant chemoradiotherapy plus surgery versus active surveillance for oesophageal cancer: a stepped-wedge cluster randomised trial. BMC Cancer. 2018;18(1):142. - PMC - PubMed
-
- Markar SR, Zaninotto G, Castoro C, Johar A, Lagergren P, Elliott JA, Gisbertz SS, Mariette C, Alfieri R, Huddy J, et al. Lasting Symptoms After Esophageal Resection (LASER): European Multicenter Cross-sectional Study. Ann Surg. 2020. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
