

Concurrent SMARCA4-deficient and poorly differentiated adenocarcinomas in separate lung lobes: a case report and literature review
- PMID: 40405273
- PMCID: PMC12096594
- DOI: 10.1186/s12957-025-03839-6
Concurrent SMARCA4-deficient and poorly differentiated adenocarcinomas in separate lung lobes: a case report and literature review
Abstract
Background: SMARCA4 and SMARCA2, mutually exclusive catalytic ATPase subunits of human mammalian Switch/Sucrose-Nonfermentable chromatin remodeling enzymes, function as tumor suppressor genes. SMARCA4-deficient adenocarcinoma (SMARCA4-dADC) is a relatively rare subtype of TTF1/P40-negative non-small cell lung cancer. The concurrent presentation of SMARCA4-dADC and poorly differentiated adenocarcinoma with SMARCA2 (also known as BRM) loss in separate lobes of the same patient is even less common. This report describes such a case involving the simultaneous occurrence of these two tumor types in distinct locations within the lungs.
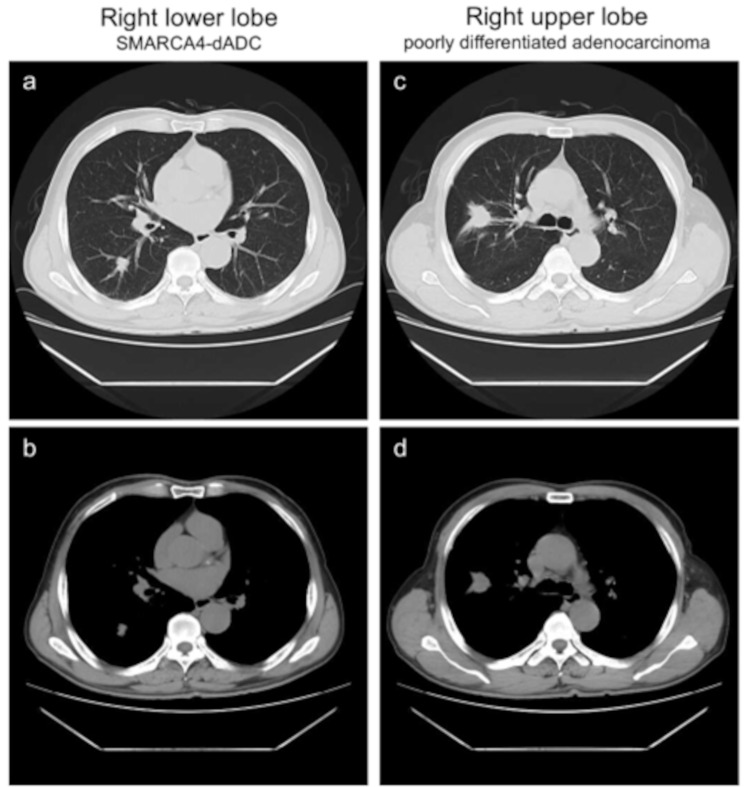
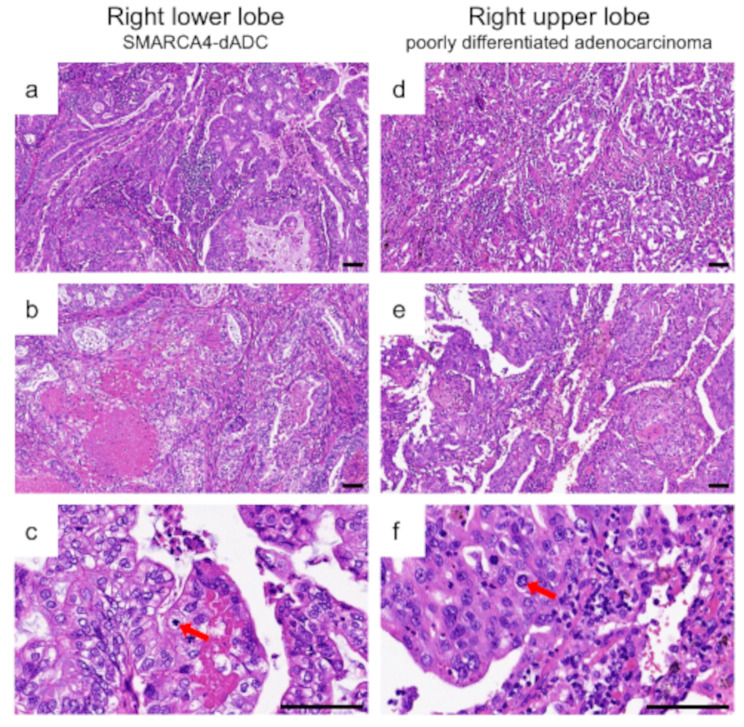
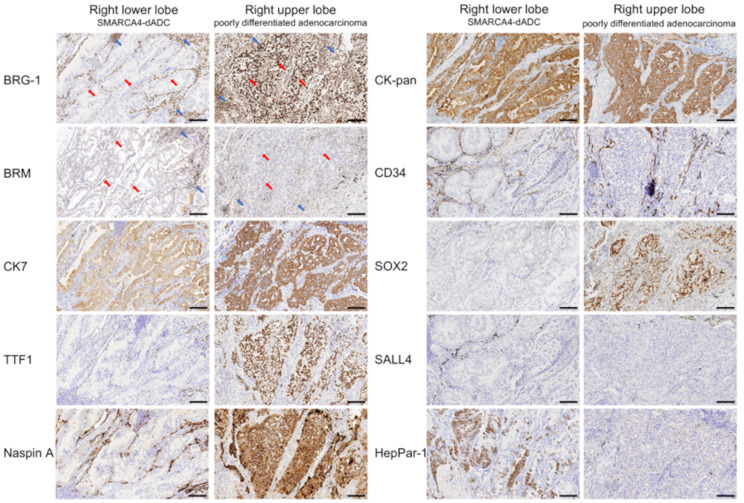
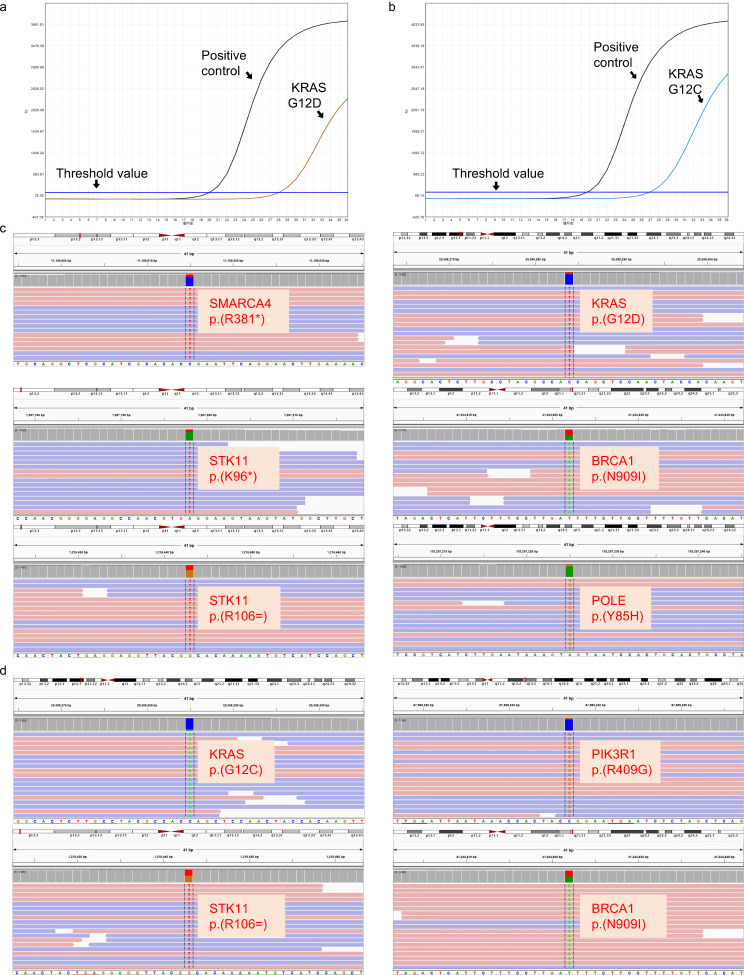
Case presentation: A 68-year-old male presented with a three-week history of vague pain in the right side of the chest, with no obvious trigger. Imaging revealed solid masses in the upper and lower lobes of the right lung with bilateral enlarged cervical lymph nodes. So, both of these masses underwent wedge resection. Histopathological examination confirmed that the lower lobe tumor was SMARCA4-dADC, while the upper lobe tumor was diagnosed as poorly differentiated adenocarcinoma. Although histologically similar, both exhibiting predominantly solid sheets and complex glandular structures, the two tumors displayed distinct immunohistochemical and molecular profiles. The lower lobe mass showed complete loss of BRG1 protein expression and partial loss of BRM. Immunohistochemical analysis revealed negative expression of TTF1, Napsin A, SALL4, CD34, and SOX2, and positive expression of CK7, pan-Cytokeratin (CK-pan), and HepPar-1. Molecular analysis identified mutations in SMARCA4, KRAS, and STK11. Conversely, the upper lobe mass retained BRG1 expression but showed complete loss of BRM protein expression, and negative expression of SALL4, CD34, and HepPar-1, positive expression of CK7, CK-pan, TTF1, Napsin A, and SOX2. A KRAS mutation was also detected in this tumor.
Conclusion: The simultaneous occurrence of SMARCA4-dADC and conventional adenocarcinoma in different locations within the same patient is exceedingly rare. However, the distinct immunophenotypic and molecular characteristics of SMARCA4-dADC differentiate it as a unique entity from conventional adenocarcinoma. We recommend including SMARCA4 in the marker panel used to evaluate TTF1-negative adenocarcinomas of potential or uncertain pulmonary origin. This report underscores the diagnostic challenge of concurrent SMARCA4-dADC and poorly differentiated adenocarcinoma, proposing a standardized immunohistochemical workflow to guide therapeutic decisions.
Keywords: Brahma-related gene 1 (BRG1) protein; Non-small cell lung cancers; SMARCA2; SMARCA4.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics: The research was approved by the institutional ethics review board of the Fourth Affiliated Hospital, Zhejiang University School of Medicine (K2025006) and conducted in accordance with the principles of the World Medical Association’s Declaration of Helsinki “Ethical Principles for Medical Research Involving Human Beings.” Informed consent: Written informed consent was obtained from the patient to publish this paper. Conflict of interest: The authors declare no conflict of interest.
Figures
Similar articles
-
SMARCA4-deficient pulmonary adenocarcinoma: clinicopathological, immunohistochemical, and molecular characteristics of a novel aggressive neoplasm with a consistent TTF1neg/CK7pos/HepPar-1pos immunophenotype.Virchows Arch. 2017 Nov;471(5):599-609. doi: 10.1007/s00428-017-2148-5. Epub 2017 May 30. Virchows Arch. 2017. PMID: 28555282
-
SMARCA4 and SMARCA2 deficiency in non-small cell lung cancer: immunohistochemical survey of 316 consecutive specimens.Ann Diagn Pathol. 2017 Feb;26:47-51. doi: 10.1016/j.anndiagpath.2016.10.006. Epub 2016 Oct 20. Ann Diagn Pathol. 2017. PMID: 28038711
-
SMARCA4/BRG1-Deficient Non-Small Cell Lung Carcinomas: A Case Series and Review of the Literature.Arch Pathol Lab Med. 2021 Jan 1;145(1):90-98. doi: 10.5858/arpa.2019-0633-OA. Arch Pathol Lab Med. 2021. PMID: 33367658 Review.
-
SMARCA4-Deficient Thoracic Sarcoma: A Case Report and Review of Literature.Int J Surg Pathol. 2020 Feb;28(1):102-108. doi: 10.1177/1066896919865944. Epub 2019 Aug 5. Int J Surg Pathol. 2020. PMID: 31382829 Review.
-
Case Report: FAP+ fibroblasts and SPP1+ macrophages in SMARCA2-deficient while SMARCA4-preserved poorly differentiated lung adenocarcinoma: two case reports and multi-omics analysis.Front Immunol. 2025 May 16;16:1568556. doi: 10.3389/fimmu.2025.1568556. eCollection 2025. Front Immunol. 2025. PMID: 40453096 Free PMC article.
References
-
- Perret R, Chalabreysse L, Watson S, Serre I, Garcia S, Forest F, et al. SMARCA4-deficient thoracic sarcomas: clinicopathologic study of 30 cases with an emphasis on their nosology and differential diagnoses. Am J Surg Pathol. 2019;43:455–65. - PubMed
-
- Nicholson AG, Tsao MS, Beasley MB, Borczuk AC, Brambilla E, Cooper WA, et al. The 2021 WHO classification of lung tumors: impact of advances since 2015. J Thorac Oncol. 2022;17:362–87. - PubMed
-
- Sun T, Gilani SM, Podany P, Harigopal M, Zhong M, Wang H. Cytomorphologic features of SMARCA4-deficient non-small cell lung carcinoma and correlation with immunohistochemical and molecular features. Cancer Cytopathol. 2022;130:620–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
