

Impact of the presence of a prosthetic implant and transition to oral stepdown therapy on relapse rates and mortality in uncomplicated Staphylococcus aureus bacteremia treated with 14 days of antibiotics: a retrospective cohort study
- PMID: 40407372
- PMCID: PMC12211085
- DOI: 10.1128/spectrum.03337-24
Impact of the presence of a prosthetic implant and transition to oral stepdown therapy on relapse rates and mortality in uncomplicated Staphylococcus aureus bacteremia treated with 14 days of antibiotics: a retrospective cohort study
Abstract
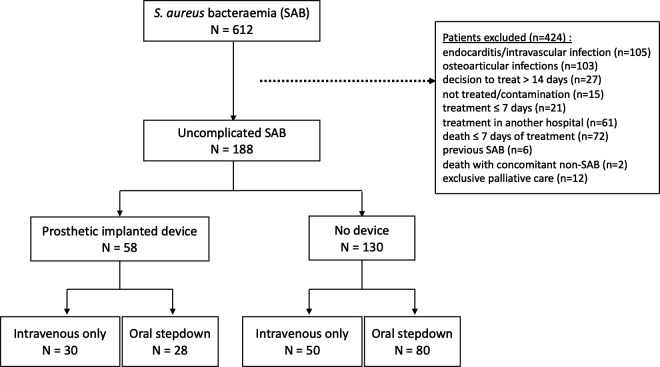
The aim of this single-center, retrospective observational study was to evaluate the effects of having a prosthetic implant (PI) and of changing from intravenous to oral antibiotics (oral stepdown therapy [OST]) on the risk of relapse in patients with otherwise uncomplicated Staphylococcus aureus bacteremia (SAB) treated with antibiotics for 14 days. The primary outcome was the 90-day SAB relapse rate in patients with and without a PI. Secondary outcomes were 90-day mortality among patients with or without a PI and 90-day SAB relapse and mortality in patients who had OST. We included 188 consecutive patients with SAB without metastatic foci and with a planned antibiotic treatment duration of 14 days: 58 (31%) had a presumed uninfected PI, and 108 (57%) had OST. Four patients (2%) relapsed, and 25 patients (13%) died. Patients with a PI were more likely to have diagnostic tests performed. In the univariate analysis, the presence of a PI (odds ratio [OR] 7 [95% confidence interval {CI} 0.9-144.0]) and OST (OR 0.7 [95% CI 0.1-6.2]) were not associated with 90-day relapse. In the multivariable analysis, the presence of a PI (adjusted odds ratio [aOR] 1.3 [95% CI 0.5-3.7]) and OST (aOR 0.5 [95% CI 0.2-1.4]) were not predictive of 90-day mortality. In a setting where full diagnostic workup and close follow-up can be ensured, the presence of a PI and OST did not seem to be associated with an increase in 90-day mortality in patients with otherwise uncomplicated SAB. Although the relapse rate was low overall, there was a non-significant trend toward a higher risk of relapse in patients with a PI.IMPORTANCEThis retrospective study provides reassuring real-world data supporting a short 14-day treatment course for SAB in patients with PIs. In an era of increasing antimicrobial resistance worldwide, these retrospective findings support the perspective that not all PIs are systematically infected. Prolonged antibiotic therapy may therefore not be routinely needed if infection is excluded and thorough evaluation for dissemination performed, accompanied by close clinical and biological monitoring. Early transition to oral therapy in this context, which has been implemented in our institution for years, does not appear to be associated with a higher risk of therapeutic failure. These findings align with the most recent literature on the subject.
Keywords: Staphylocococcus aureus; device; oral stepdown therapy; prosthesis; short-course antibiotic therapy.
Conflict of interest statement
J.-L.M. is a member of the scientific committee of the BioAster Company and has participated in advisory boards with MSD Merck Sharp & Dohme AG.
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Antibiotic strategies for eradicating Pseudomonas aeruginosa in people with cystic fibrosis.Cochrane Database Syst Rev. 2017 Apr 25;4(4):CD004197. doi: 10.1002/14651858.CD004197.pub5. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2023 Jun 2;6:CD004197. doi: 10.1002/14651858.CD004197.pub6. PMID: 28440853 Free PMC article. Updated.
-
Systemic and topical antibiotics for chronic rhinosinusitis.Cochrane Database Syst Rev. 2016 Apr 26;4(4):CD011994. doi: 10.1002/14651858.CD011994.pub2. Cochrane Database Syst Rev. 2016. PMID: 27113482 Free PMC article.
-
Different antibiotic treatments for group A streptococcal pharyngitis.Cochrane Database Syst Rev. 2023 Nov 15;11(11):CD004406. doi: 10.1002/14651858.CD004406.pub6. Cochrane Database Syst Rev. 2023. PMID: 37965935 Free PMC article.
-
Immunostimulants versus placebo for preventing exacerbations in adults with chronic bronchitis or chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2022 Nov 14;11(11):CD013343. doi: 10.1002/14651858.CD013343.pub2. Cochrane Database Syst Rev. 2022. PMID: 36373977 Free PMC article.
References
-
- Ikuta KS, Swetschinski LR, Robles Aguilar G, Sharara F, Mestrovic T, Gray AP, Davis Weaver N, Wool EE, Han C, Gershberg Hayoon A, et al. 2022. Global mortality associated with 33 bacterial pathogens in 2019: a systematic analysis for the global burden of disease study 2019. Lancet 400:2221–2248. doi: 10.1016/S0140-6736(22)02185-7 - DOI - PMC - PubMed
-
- Nambiar K, Seifert H, Rieg S, Kern WV, Scarborough M, Gordon NC, Kim HB, Song K-H, Tilley R, Gott H, Liao C-H, Edgeworth J, Nsutebu E, López-Cortés LE, Morata L, Walker AS, Thwaites G, Llewelyn MJ, Kaasch AJ, International Staphylococcus aureus collaboration (ISAC) study group (with linked authorship to members in the Acknowledgements) and the ESCMID Study Group for Bloodstream Infections and Sepsis (ESGBIS) . 2018. Survival following Staphylococcus aureus bloodstream infection: a prospective multinational cohort study assessing the impact of place of care. J Infect 77:516–525. doi: 10.1016/j.jinf.2018.08.015 - DOI - PubMed
-
- Liu Catherine, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL, Karchmer AW, Levine DP, Murray BE, Rybak MJ, Talan DA, Chambers HF. 2011. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis 52:e18–e55. doi: 10.1093/cid/ciq146 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
