

Predictive value of early DCE and DSC perfusion MRI parameters for midterm clinical outcomes in lung cancer brain metastases treated with stereotactic radiosurgery
- PMID: 40408063
- PMCID: PMC12198322
- DOI: 10.1007/s11060-025-05054-5
Predictive value of early DCE and DSC perfusion MRI parameters for midterm clinical outcomes in lung cancer brain metastases treated with stereotactic radiosurgery
Abstract
Purpose: Stereotactic Radiosurgery (SRS) is an effective way of controlling the brain metastasis (BM) of lung carcinoma. This study evaluates the performance of dynamic contrast-enhanced MRI (DCE-MRI) and dynamic susceptibility contrast MRI (DSC-MRI) parameters to distinguish responders from non-responders at midterm follow-up in lung carcinoma BMs.
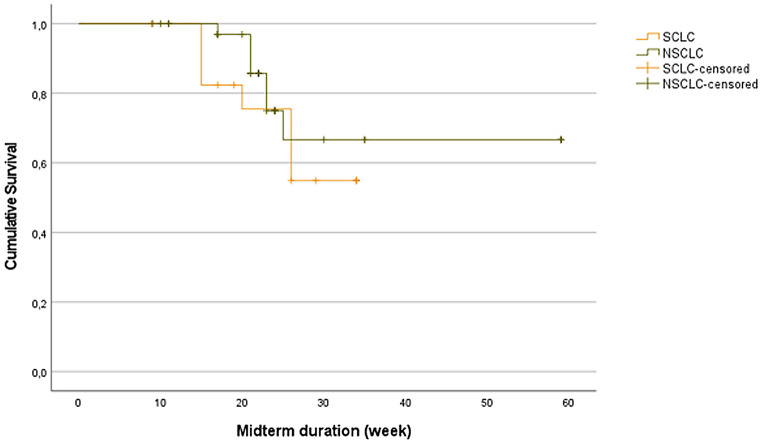
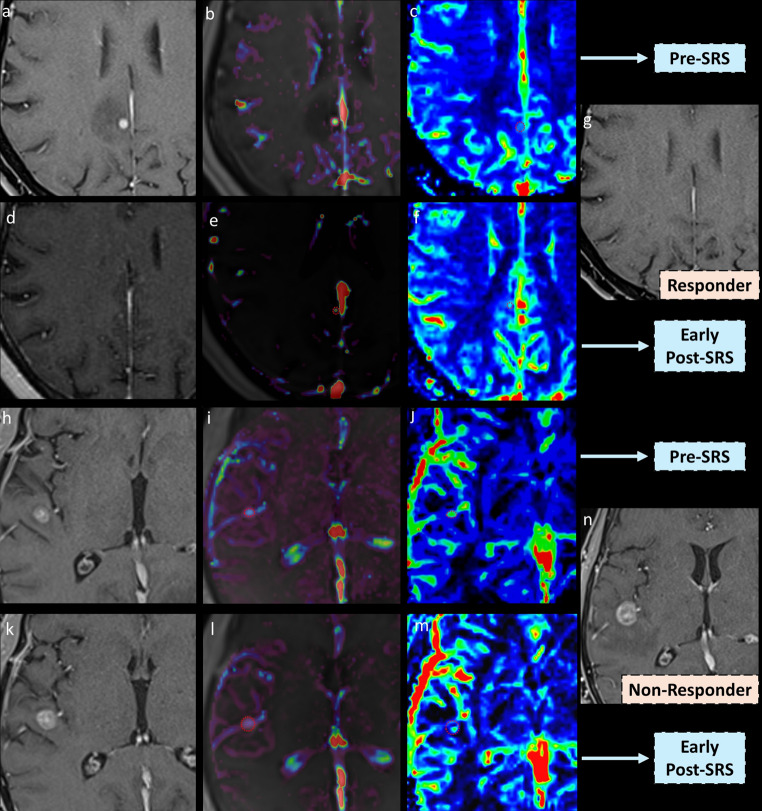
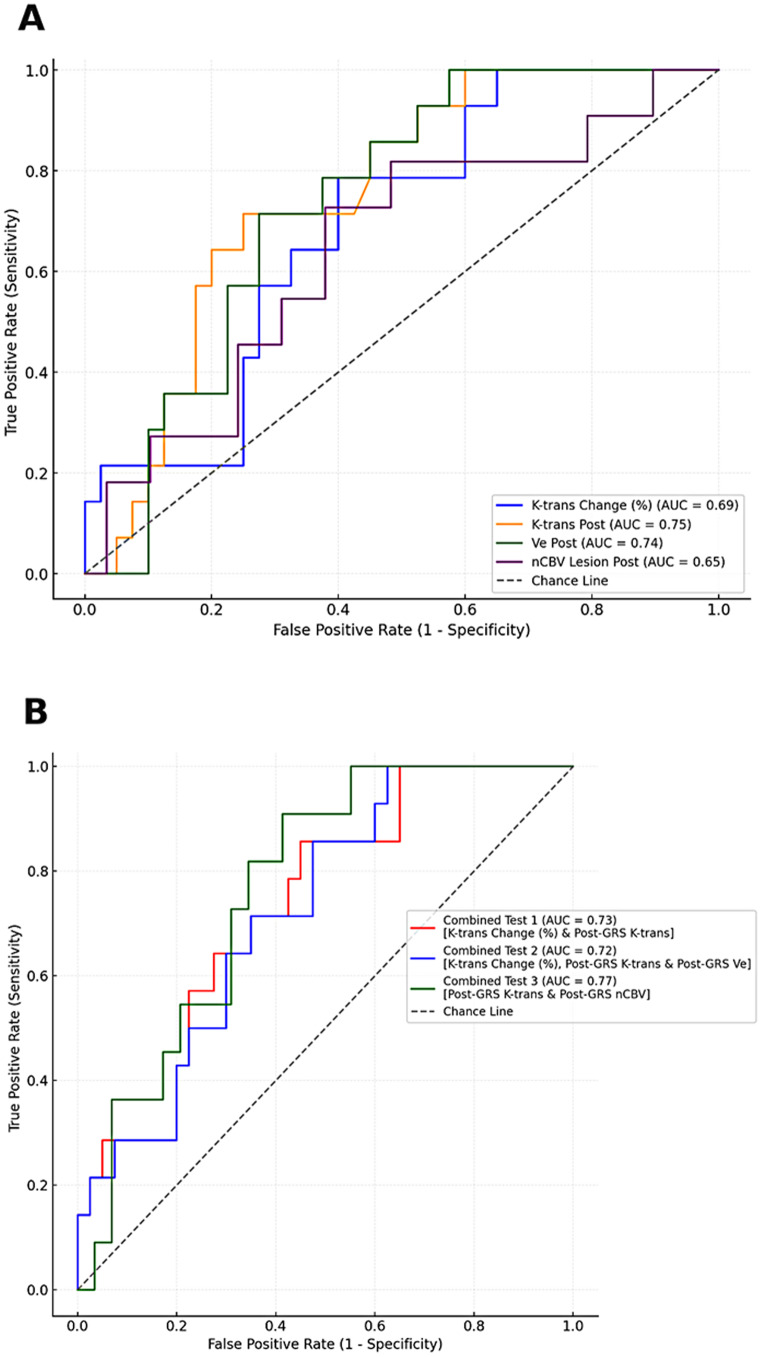
Methods: Twenty-six patients (mean age 62 ± 10 years) with 54 lung carcinoma BMs (NSCLC 67%, SCLC 33%) underwent SRS. The DCE-MRI and DSC-MRI were performed at baseline and repeated 4-8 weeks post-SRS to predict treatment responses at the midterm follow-up (6-12 months). Midterm outcomes were classified according to RANO-BM criteria as responders (complete response, partial response, or stable disease) or non-responders (progressive disease). Receiver operating characteristic (ROC) analyses evaluated the diagnostic accuracy of individual perfusion parameters and their combinations.
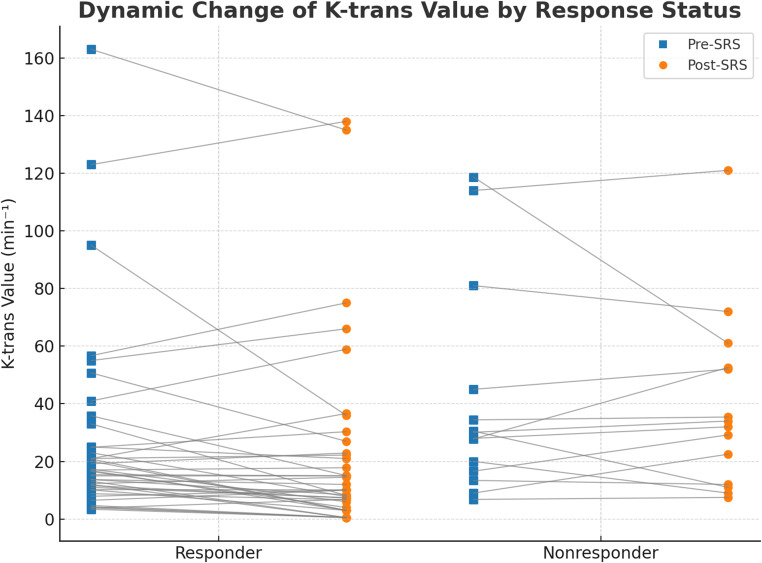
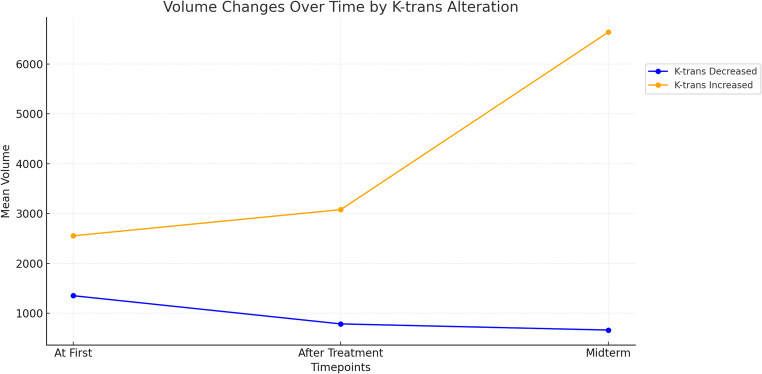
Results: Forty lesions (74%) were responders, while 14 (26%) were non-responders. Progressive lesions showed a mean volume increase of 5.5-fold, whereas responders demonstrated a 60% mean volume reduction. Responders showed significantly lower absolute post-SRS K-trans (median 0.015 vs. 0.035 min⁻¹; p = 0.005), a higher proportional decrease in K-trans from baseline (- 27% vs. +13%; p = 0.017), and lower post-SRS Ve (p = 0.009) compared to non-responders. Absolute post-SRS K-trans had the highest individual predictive accuracy (AUC = 0.75, accuracy = 78%, sensitivity = 86%, specificity = 55%). Neither the dynamic change nor post-SRS nCBV alone predicted midterm response; however, combining post-SRS nCBV with K-trans slightly improved predictive performance (AUC = 0.76, accuracy = 79%).
Conclusion: Early post-SRS absolute K-trans is the best perfusion parameter for predicting midterm response in lung carcinoma BMs. DSC-MRI parameters alone offer limited predictive value.
Keywords: Brain metastasis; Lung carcinoma; Perfusion MRI; Stereotactic radiosurgery.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Non-interventional Clinical Research Ethics Committee of Koc University under reference 2025.100.IRB2.047. Informed consent: Signed informed consent was waived from all individual participants included in the study. Competing interests: The authors declare no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
