

Single-cell multimodal analysis reveals tumor microenvironment predictive of treatment response in non-small cell lung cancer
- PMID: 40408481
- PMCID: PMC12101509
- DOI: 10.1126/sciadv.adu2151
Single-cell multimodal analysis reveals tumor microenvironment predictive of treatment response in non-small cell lung cancer
Abstract
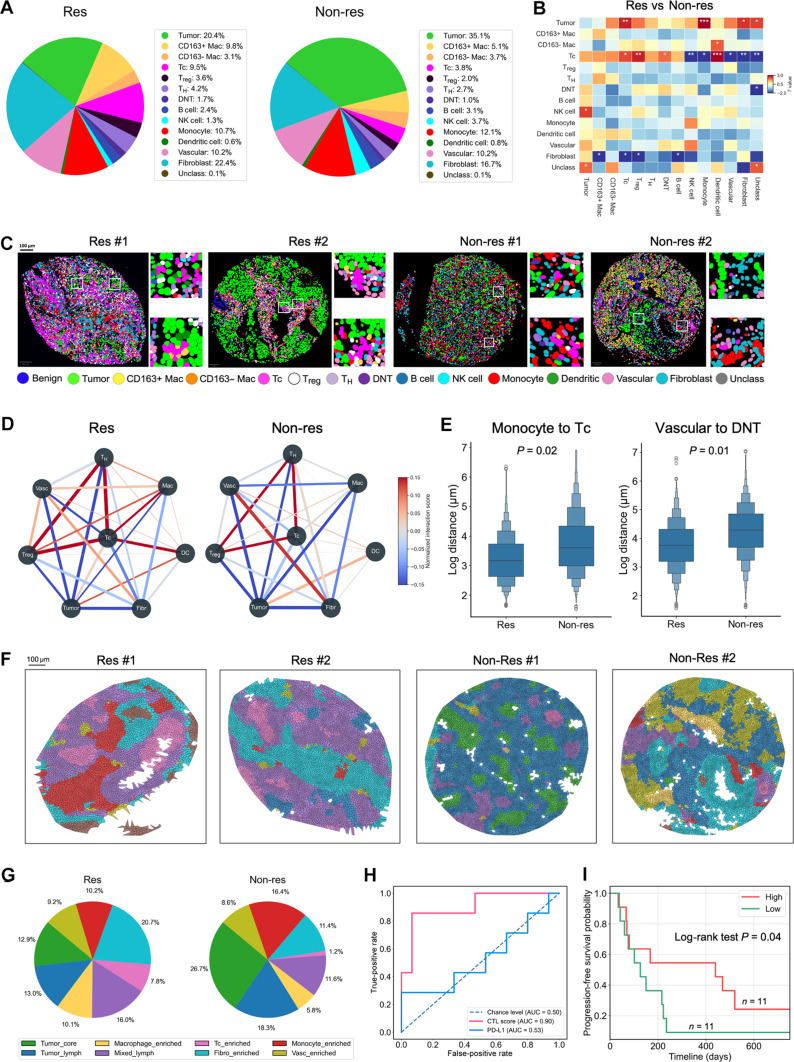
Non-small cell lung cancer (NSCLC) constitutes over 80% of lung cancer cases and remains a leading cause of cancer-related mortality worldwide. Despite the advent of immune checkpoint inhibitors, their efficacy is limited to 27 to 45% of patients. Identifying likely treatment responders is essential for optimizing healthcare and improving quality of life. We generated multiplex immunofluorescence (mIF) images, histopathology, and RNA sequencing data from human NSCLC tissues. Through the analysis of mIF images, we characterized the spatial organization of 1.5 million cells based on the expression levels for 33 biomarkers. To enable large-scale characterization of tumor microenvironments, we developed NucSegAI, a deep learning model for automated nuclear segmentation and cellular classification in histology images. With this model, we analyzed the morphological, textural, and topological phenotypes of 45.6 million cells across 119 whole-slide images. Through unsupervised phenotype discovery, we identified specific lymphocyte phenotypes predictive of immunotherapy response. Our findings can improve patient stratification and guide selection of effective therapeutic regimens.
Figures




References
-
- Arriagada R., Bergman B., Dunant A., Le Chevalier T., Pignon J.-P., Vansteenkiste J., International Adjuvant Lung Cancer Trial Collaborative Group , Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer. N. Engl. J. Med. 350, 351–360 (2004). - PubMed
-
- al-Kattan K., Sepsas E., Fountain S. W., Townsend E. R., Disease recurrence after resection for stage I lung cancer. Eur. J. Cardiothorac. Surg. 12, 380–384 (1997). - PubMed
-
- Alberts W. M., Follow up and surveillance of the patient with lung cancer: What do you do after surgery? Respirology 12, 16–21 (2007). - PubMed
-
- Zimmermann F. B., Molls M., Jeremic B., Treatment of recurrent disease in lung cancer. Semin. Surg. Oncol. 21, 122–127 (2003). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
