

Continuation vs Withdrawal of Beta-Blockers and Outcomes After Myocardial Infarction With Preserved Left Ventricular Function
- PMID: 40408795
- PMCID: PMC12152613
- DOI: 10.1016/j.jacadv.2025.101814
Continuation vs Withdrawal of Beta-Blockers and Outcomes After Myocardial Infarction With Preserved Left Ventricular Function
Abstract
Background: The role of routine beta-blocker (BB) use after uncomplicated acute myocardial infarction (AMI) treated with contemporary therapies is not well established.
Objectives: The authors conducted a retrospective cohort study using linked registry and administrative data to evaluate whether early BB discontinuation (a prescription ending within 180 days of discharge) is associated with clinical outcomes.
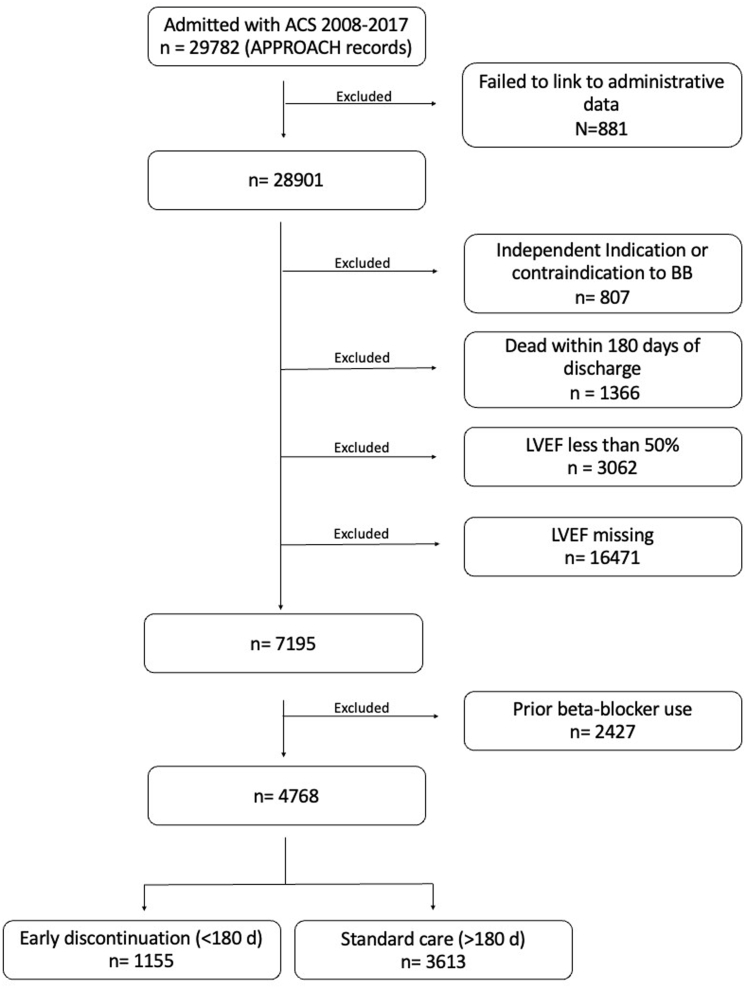
Methods: We included patients who survived at least 180 days after AMI from 2008 to 2017 with new BB prescription and left ventricular ejection fraction ≥50%. The primary outcome was a composite of recurrent AMI, myocardial revascularization, or all-cause mortality within 5 years. Secondary outcomes were each of the components of the composite. Cox proportional hazard models were used to evaluate the association between early BB discontinuation and outcomes.
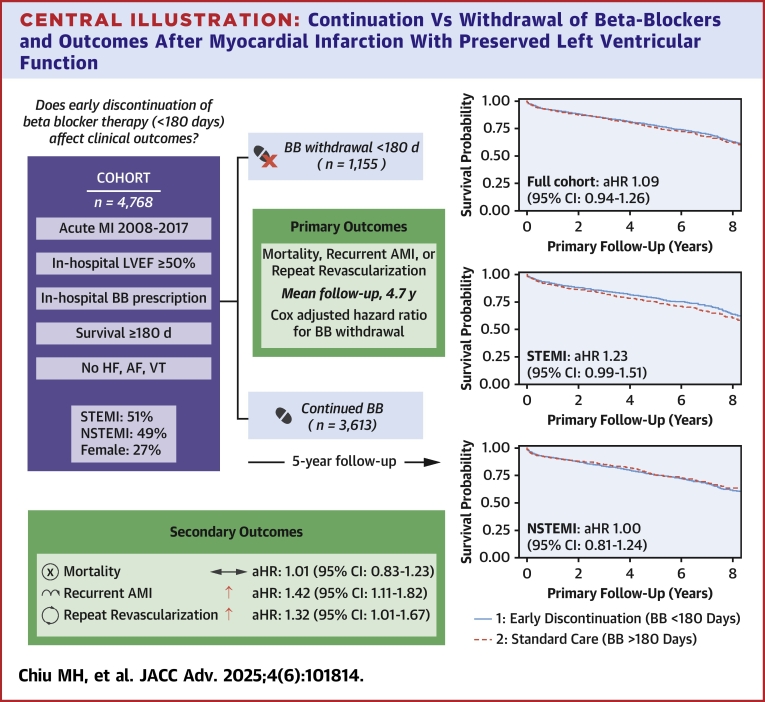
Results: Among the 4,768 included patients, 1,155 (24.2%) discontinued BB within 180 days of AMI discharge. During a median follow-up time of 57 months, 964 patients (20.2%) experienced the primary outcome. Early BB discontinuation was not associated with an increased risk of the primary outcome (adjusted HR: 1.09; 95% CI: 0.94-1.26), or with all-cause mortality (HR: 1.04; 95% CI: 0.86-1.26). However, early BB discontinuation was associated with an increased risk for recurrent AMI and a higher rate of repeat revascularization.
Conclusions: In patients with preserved left ventricular ejection fraction after AMI, discontinuation of BB within 180 days was not associated with a significantly increased risk of a composite outcome of death, recurrent AMI, or revascularization but was associated with increased risk of recurrent AMI and need for repeat revascularization.
Keywords: acute myocardial infarction; beta-blocker; mortality.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding support and author disclosures Funding was provided by the Libin Cardiac Institute's Clinical Research Development Fund. AbSPORU is supported by CIHR, Alberta Innovates, the University Hospital Foundation, and in-kind contributions from AHS, WCHRI, ACHRI, and the Universities of Alberta and Calgary. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures

References
-
- O’Gara P.T., Kushner F.G., Ascheim D.D., et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. Circulation. 2013;127(4):e362–e425. - PubMed
-
- Amsterdam E.A., Wenger N.K., Brindis R.G., et al. 2014 AHA/ACC guideline for the management of patients with non–ST-elevation acute coronary syndromes. J Am Coll Cardiol. 2014;64(24):e139–e228. - PubMed
-
- Yusuf S., Peto R., Lewis J., Collins R., Sleight P. Beta blockade during and after myocardial infarction: an overview of the randomized trials. Prog Cardiovasc Dis. 1985;27(5):335–371. - PubMed
-
- Olsson G., Rehnqvist N. Evaluation of antiarrhythmic effect of metoprolol treatment after acute myocardial infarction: relationship between treatment responses and survival during a 3-year follow-up. Eur Heart J. 1986;7(4):312–319. - PubMed
-
- Group B.R. A randomized trial of propranolol in patients with acute myocardial infarction. JAMA. 1982;247:1707. - PubMed
LinkOut - more resources
Full Text Sources
