

Jugular Vein Intracardiac Echocardiography-Guided Percutaneous Transluminal Septal Myocardial Ablation: A Novel Approach in 4 Cases
- PMID: 40409849
- PMCID: PMC12243039
- DOI: 10.1016/j.jaccas.2025.103307
Jugular Vein Intracardiac Echocardiography-Guided Percutaneous Transluminal Septal Myocardial Ablation: A Novel Approach in 4 Cases
Abstract
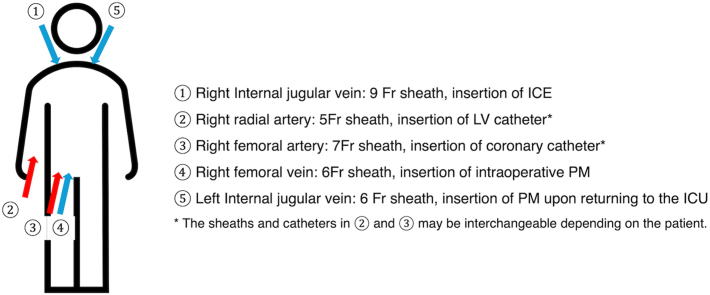
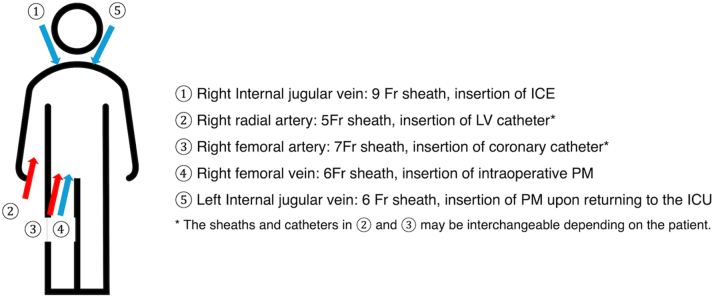
Objective: This study sought to describe a novel technique for percutaneous transluminal septal myocardial ablation using intracardiac echocardiography (ICE) through the right internal jugular vein (JV) in patients with hypertrophic obstructive cardiomyopathy.
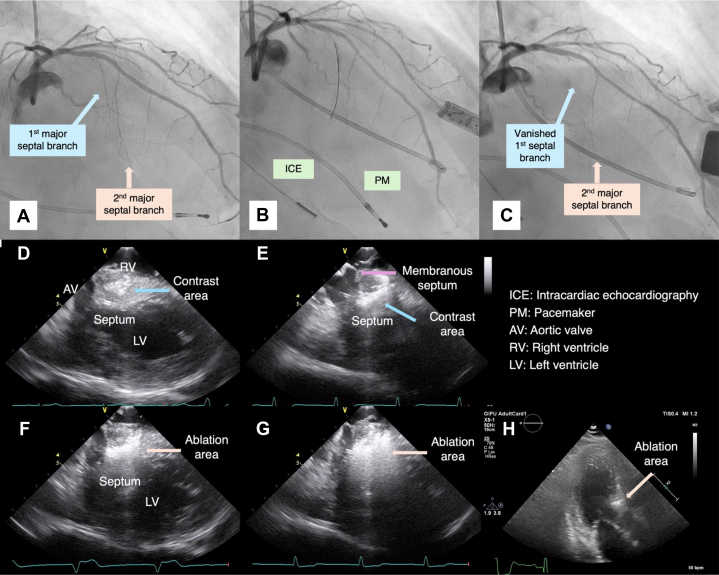
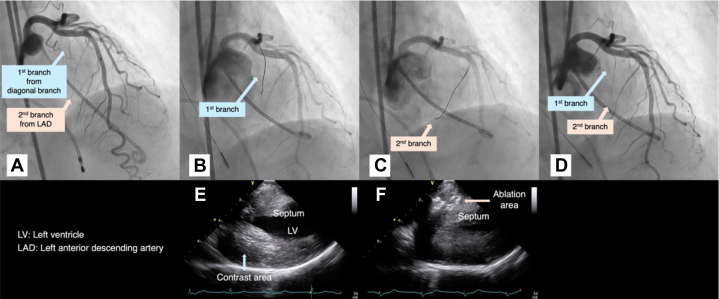
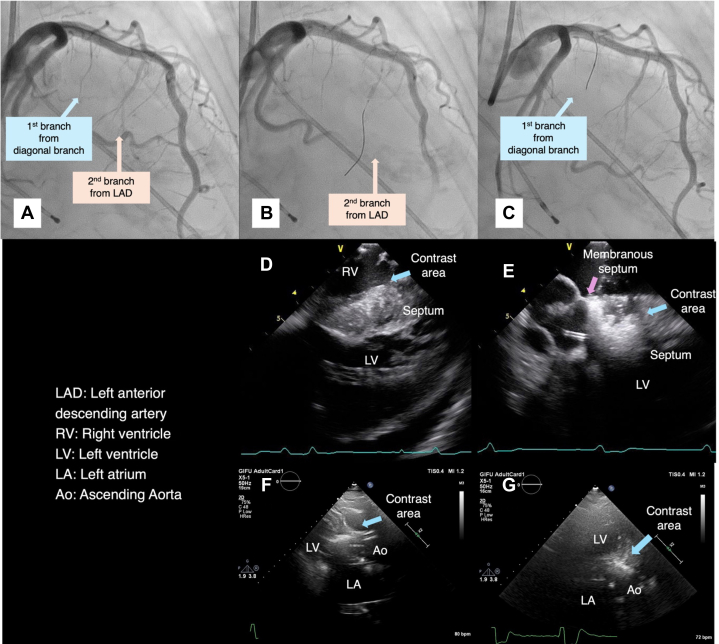
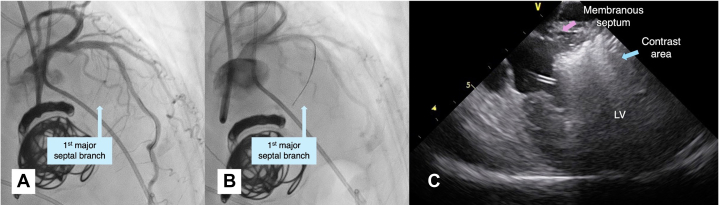
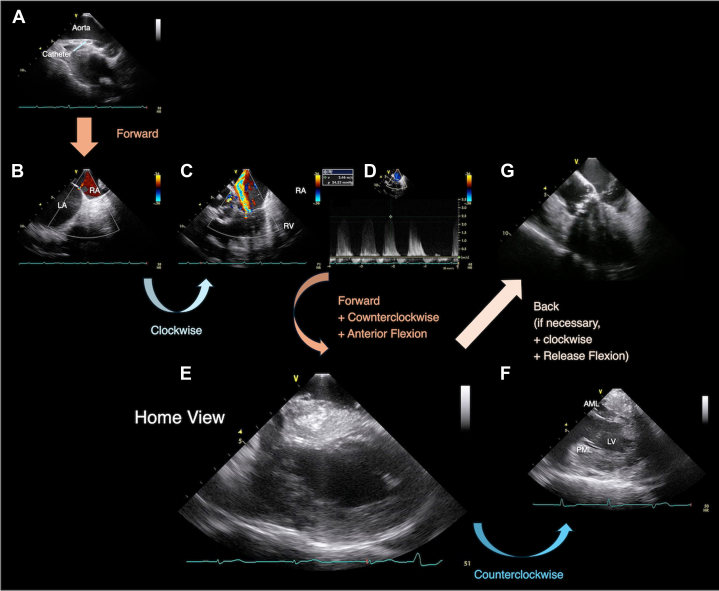
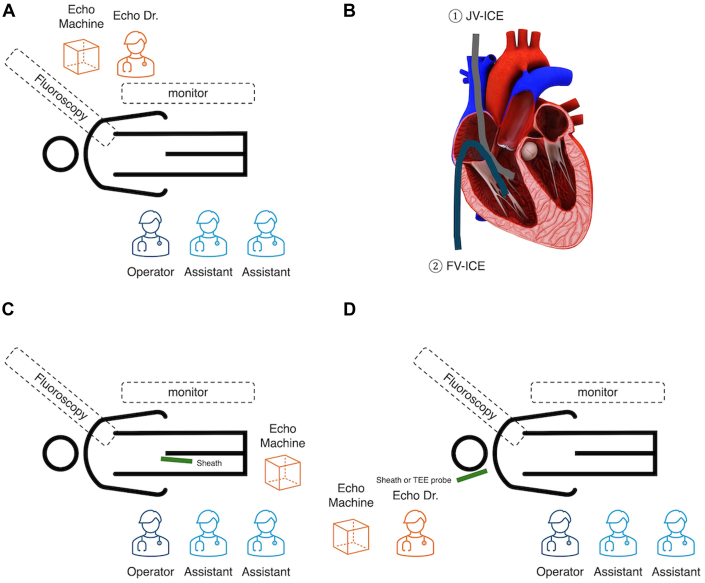
Key steps: Prepare the equipment and establish vascular access, insert the JV ICE catheter using a sterile sleeve, perform initial screening with JV ICE to obtain key cardiac views, identify target septal branch using coronary angiography and JV ICE, monitor contrast injection and ethanol administration in real time with JV ICE, continuously assess for immediate complications, and evaluate postprocedure gradient reduction and ablation efficacy.
Potential pitfalls: Risks include vascular complications, arrhythmias, cardiac tamponade, embolism, and infections. JV ICE requires specific skills, presenting a learning curve. Mitigation strategies involve ultrasound-guided access, careful catheter manipulation, strict asepsis, comprehensive training, optimized settings, and continuous monitoring.
Keywords: cardiomyopathy; echocardiography; treatment.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Yagasaki has received MitraClip proctorship fees from Abbott Medical Japan that are not directly related to the content of this paper. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures

Similar articles
-
Alcohol septal ablation for hypertrophic obstructive cardiomyopathy: a systematic review of published studies.J Interv Cardiol. 2006 Aug;19(4):319-27. doi: 10.1111/j.1540-8183.2006.00153.x. J Interv Cardiol. 2006. PMID: 16881978
-
Ultrasound guidance versus anatomical landmarks for internal jugular vein catheterization.Cochrane Database Syst Rev. 2015 Jan 9;1(1):CD006962. doi: 10.1002/14651858.CD006962.pub2. Cochrane Database Syst Rev. 2015. PMID: 25575244 Free PMC article.
-
Venous cutdown versus the Seldinger technique for placement of totally implantable venous access ports.Cochrane Database Syst Rev. 2016 Aug 21;2016(8):CD008942. doi: 10.1002/14651858.CD008942.pub2. Cochrane Database Syst Rev. 2016. PMID: 27544827 Free PMC article.
-
A pilot study on coronary microvascular dysfunction in obstructive hypertrophic cardiomyopathy: impact of percutaneous transluminal septal myocardial ablation.Cardiovasc Interv Ther. 2025 Jun 27. doi: 10.1007/s12928-025-01154-1. Online ahead of print. Cardiovasc Interv Ther. 2025. PMID: 40576939
-
Intracardiac versus transesophageal echocardiographic guidance for left atrial appendage occlusion: Design and rationale of the ICE-TEE trial.Cardiovasc Revasc Med. 2025 Jun 1:S1553-8389(25)00282-9. doi: 10.1016/j.carrev.2025.05.029. Online ahead of print. Cardiovasc Revasc Med. 2025. PMID: 40579293
References
-
- Writing Committee Members, Ommen S.R., Ho C.Y., et al. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2024;83:2324–2405. - PubMed
-
- Maron M.S., Olivotto I., Zenovich A.G., et al. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation. 2006;114:2232–2239. - PubMed
-
- Faber L., Seggewiss H., Gleichmann U. Percutaneous transluminal septal myocardial ablation in hypertrophic obstructive cardiomyopathy: results with respect to intraprocedural myocardial contrast echocardiography. Circulation. 1998;98(22):2415–2421. - PubMed
-
- Monakier D., Woo A., Puri T., et al. Usefulness of myocardial contrast echocardiographic quantification of risk area for predicting postprocedural complications in patients undergoing septal ethanol ablation for obstructive hypertrophic cardiomyopathy. Am J Cardiol. 2004;94(12):1515–1522. - PubMed
-
- Pedone C., Vijayakumar M., Ligthart J.M.L., et al. Intracardiac echocardiography guidance during percutaneous transluminal septal myocardial ablation in patients with obstructive hypertrophic cardiomyopathy. Int J Cardiovasc Intervent. 2005;7(3):134–137. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
